Carpal dislocations
Introduction
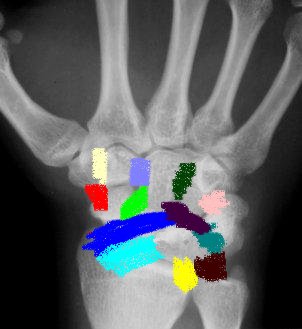
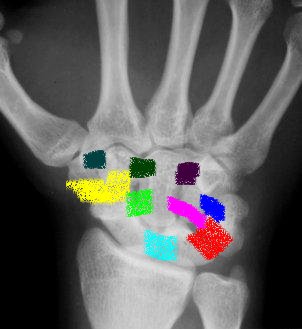
Lunate and perilunate dislocations although rare in themselves, they are the most common carpal dislocations.
The terminology around lunate and perilunate dislocations can be a little confusing.
-
Lunate dislocation - This is where the lunate bone dislocates out of the radiocarpal joint, normally volarly.
-
Perilunate dislocation - This is where the lunate remains in the radiocarpal joint (lunate fossa) and the rest of the carpus dislocates around the lunate, normally dorsally.
There are several variants of perilunate dislocation depending on where the force has gone and the structures injured eg:
-
Transcaphoid perilunate dislocation - here the force enters the carpus through and fracturing the scaphoid travels laterally usually disrupting the lunotriquetral LT ligament. The significance here is the Scapholunate Ligament SL is usually remains intact.
-
Transtyloid perilunate dislocation - here the force enters via the radial styloid, progresses through the SL ligament around the Lunate and exits again via the LT ligament.
It is important to appreciate the path of the energy as, critical to a good outcome is open reduction and repair of the injured structures.
Median nerve compression occurs in 25% of cases, if present emergency reduction is required.
It is worth undertaking a preliminary reduction of the carpus in the Emergency department under sedation, closed reduction and cast immobilisation may not be the definitive treatment, but once reduced definitive fixation may follow once facilities and expertise is available.
Classification
Mayfield described the 4 stages of ligament injury progressing round the lunate ultimately leading to a lunate dislocation
 Volar
extrinsic Volar
extrinsic |
 Intrinsic Intrinsic |
|
|
Treatment
Several treatment options exist to treat perilunar instability patterns
-
Closed reduction and cast immobilization
-
Closed reduction and percutaneous k wires
-
Open reduction , single and combined approaches with protection of repair with K wires or screws or interosseous cerclage wiring
All the approaches above have a place in the treatment.
The trend is to be more aggresive and attempt open repair of the injured structures bony and ligamentous (extrinsic and intrinsic) through combined volar and dorsal approaches.
If a closed reduction of a perilunate or a lunate dislocation can be achieved and held in a backslab and no median nerve injury is present. Open reduction repair and protection of the repair may be performed semi urgently within a week by an experienced surgeon.
If acute carpal tunnel syndrome is diagnosed, emergent reduction and carpal tunnel decompression should be performed.
Closed reduction
Requires adequate sedation (see sedation)
Apply longitudinal traction manual or via finger traps with 15 pounds of weight, for a minimum of 10 minutes.
Obtain radiographs while applying traction this will often show associated carpal fractures not initially visualized.
To reduce a perilunate dislocation hyperextend the wrist and apply a dorsally directed force over the lunate keeping the lunate reduced. Gradually flex the wrist with a volar directed pressure over the capitate, pushing the carpus back onto lunate.
To reduce a volar lunate dislocation perform the same maneuver, although reduction of the lunate is accomplished by rotating the lunate dorsally into the lunate fossa.
Greater arc injuries may be more difficult or impossible to reduce in a closed manner.
Occasionaly it is possible to reduce closed but not hold it in a splint if so proceed to formal open reduction and internal fixation, if not skilled enough or unstable polytrauma patient temporarily K wire carpus or use external fixator to keep it reduced.
Open reduction
It is possible to treat these injuries with either volar, dorsal or combined volar and dorsal approaches.
The dorsal approach provides excellent exposure allowing accurate reduction of carpus and repair of intrinsic ligaments. It also affords good exposure for repair of bony injuries eg. scaphoid.
The volar approach allows for decompression of the carpal tunnel, reduction of a volar lunate dislocation and open repair of the volar extrinsic ligaments (radioscaphocapitate ligament).
See Approaches for Dorsal and volar approach
Complications
Perilunate dislocations of the wrist are devastating injuries.
Complications include
-
pain
-
Stiffness
-
Carpal instability
-
Post-traumatic arthritis
-
Median nerve injury
-
Weakness
References
Mayfield JK, Johnson RP, Kilcoyne RK, et al. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg [Am] 1980;5(3):226–41.
PHILIP E. BLAZAR; PETER MURRAY; Treatment of Perilunate Dislocations by Combined Dorsal and Palmar Approaches. Techniques in Hand and Upper Extremity Surgery 5(1):2–7, 2001
Page created by: Lee Van Rensburg
Last updated: 11/09/2015