Combined approach for lunate & perilunate dislocation
Indication
Lunate and perilunate dislocations (see carpal dislocation)
It may be necessary to do combined volar and dorsal approache or only volar or only dorsal (see carpal dislocation)
Anatomy
Considerations
Positioning
Supine, radiolucent hand table
Tourniquet
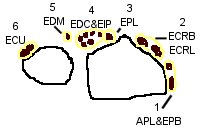
DORSAL
Skin Incision
Dorsal 10-cm longitudinal incision centred over Lister’s tubercle
Superficial dissection
Enter 3rd dorsal compartment, translocate extensor pollicis longus (EPL).
Elevate the 2nd and 4th extensor compartments subperiosteally, exposing the wrist capsule.
Several arthrotomies have been advocated to expose the radiocarpal and midcarpal joints.
If a rent already in dorsal capsule incorporate this, ensure arthrotomy generous enough to visualize scapholunate, lunotriquetral and midcarpal joints.
-
Longitudinal
-
Inverted “T”-shape
-
Radial based flap splitting and preserving dorsal ligaments (Dorsal intercarpal ligament & Dorsal radiotriquetral ligament)
 |
 |
| Inverted T | Radial based flap |
Deep dissection
Remember most of the blood supply to the scaphoid enters along its dorsal ridge, take care to preserve soft tissue attachments to the scaphoid in this region.
Remove any loose debri, bone cartilage or soft tissue. Note and record any osteochondral injuries.
If doing a combined approach now proceed to Volar approach.
VOLAR
Skin incision
Extended carpal tunnel incision

Superficial dissection
Release the transverse carpal ligament
Divide the anterior forearm fascia in line with the incision proximal to the transverse carpal ligament.
Decompress and retract the median nerve and flexor tendons.
The palmar capsule will have a transverse tear, for unreduced volar lunate dislocations the lunate will be apparent protruding through the rent in the capsule.
Reduce the lunate with traction and digital pressure. If unstable stabilize it temporarily with a K wire under direct vision through the radius. Reduce the midcarpal joint.
Reconstruction
Define the injured structures and plan repair accordingly.
Aims of reconstruction:
-
Establish and maintain the normal intracarpal anatomy
-
Reduce and securely fix any fractures (eg scaphoid or radial styloid). It is important to repair the radial styloid because of the origin of the radio-scapho-capitate ligament.
-
Repair intrinsic and extrinsic ligamentsheld with a distally directed cannulated screw (Fig. 8).
Place K wires in lunate, scaphoid and triquetrum and use them as joysticks to reduce carpal alignment.
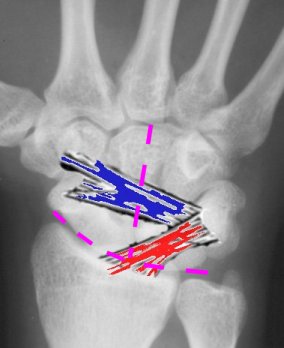
Lunotriquetral joint/ ligament
The lunotriquetral ligament is often too flimsy to repair, the triquetrum typically will assume an extended position and
needs to be flexed relative to the lunate.
Reduce and percutaneously pin the Lunotriquetral joint.
Place 2 wires across the L-T joint to prevent rotation, or one across the LT joint and a second across the midcarpal joint into the hamate. Beware of the dorsal sensory branch of the ulnar nerve.
Scapholunate joint/ ligament
Reduce and pin the SL joint with 2 wires and place one wire across the distal pole of the scaphoid into the capitate to prevent derotation. Repair the SL ligament either direct repair or with mini G2 anchor, it is often a bony avulsion from the scaphoid.
The S-L ligament repair may be reinforced by capsulodesis - use the remnants of the dorsal intercarpal ligament, detached from the triquetrum while remaining attached to the distal pole of the scaphoid. The triquetral attachment is then attached to the distal radius with suture anchors, in line with the axis of the scaphoid. (see scapholunate)
An additional wire can be placed from the radial border of the distal
radius into the lunate. This is done in a fashion similar to
that previously described for the lunate dislocation. The
radiolunate K-wire aids in reduction but is not a component of the definitive
fixation.
Asses reduction by:
-
inspecting the joint
-
Image intensifier to assess intercarpal relationships.
Guides to adequacy of reduction include coverage of the entire head of the capitate by the lunate, intracarpal interval, and the lateral scapholunate angle.
Repair transverse volar capsule with 2–0 braided, nonabsorbable suture. Repair of the volar capsule is critical, because the dorsal capsule is frequently difficult to reconstruct.
Repair the dorsal capsule and the extensor retinaculum, leaving extensor pollicis in a subcutaneous position.
Cut the pins beneath the skin.
Post operatively
Place in a backslab with wrist in “prehensile” position (15° dorsiflexion)
Once wounds and swelling settled place in thumb spica cast, remove wires at 8 weeks.
Immobilize in cast for 3 months, then use removable splint for a further 3 months
References
PHILIP E. BLAZAR; PETER MURRAY; Treatment of Perilunate Dislocations by Combined Dorsal and Palmar Approaches. Techniques in Hand and Upper Extremity Surgery 5(1):2–7, 2001