Talar neck Fractures
Aviator's astragalus hyper-dorsiflexion injury usually.
No such thing as minimally displaced grade I fracture.
High risk of AVN of the Talar body proportional to displacement.
Due to blood supply of Talus.
Anatomy
Bony anatomy
The talus consists of:
-
Body
-
Neck
-
Head
 |
The superior surface of the body presents, behind, a smooth trochlear surface for articulation with the tibia. The trochlea is broader in front than behind, convex from before backward, slightly concave from side to side: in front it is continuous with the upper surface of the neck of the bone.
|
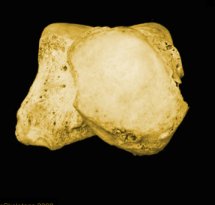
| Superior view of talus | |
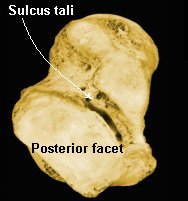 |
The inferior surface presents two articular areas, the posterior and middle calcaneal surfaces, separated from one another by a deep groove, the sulcus tali. The groove runs obliquely forward and lateralward, becoming gradually broader and deeper in front: in the articulated foot it lies above a similar groove upon the upper surface of the calcaneus, and forms, with it, a canal (sinus tarsi). The posterior calcaneal articular surface is large and it articulates with the corresponding facet on the upper surface of the calcaneus. The middle calcaneal articular surface is small, oval in form and slightly convex; it articulates with the upper surface of the sustentaculum tali of the calcaneus.
|
| Inferior view of talus | |
 |
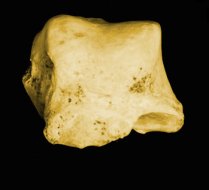
The medial surface presents at its upper part a pear-shaped articular facet for the medial malleolus, continuous above with the trochlea; below the articular surface is a rough depression for the attachment of the deep portion of the deltoid ligament of the ankle-joint. |
| Medial view | |
 |
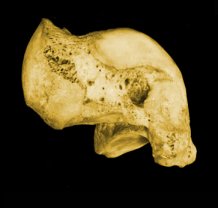
The lateral surface carries a large triangular facet, concave from above downward, for articulation with the lateral malleolus; its anterior half is continuous above with the trochlea; and in front of it is a rough depression for the attachment of the anterior talofibular ligament. Between the posterior half of the lateral border of the trochlea and the posterior part of the base of the fibular articular surface is a triangular facet which comes into contact with the transverse inferior tibiofibular ligament during flexion of the ankle-joint; below the base of this facet is a groove which affords attachment to the posterior talofibular ligament. |
| Lateral view | |
 |
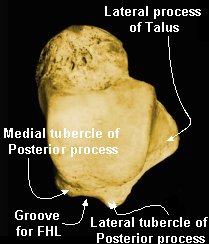
The posterior surface is narrow, and traversed by a groove running obliquely downward and medialward, and transmitting the tendon of the Flexor hallucis longus. Lateral to the groove is a prominent tubercle, the posterior process, to which the posterior talofibular ligament is attached; this process is sometimes separated from the rest of the talus, and is then known as the os trigonum. Medial to the groove is a second smaller tubercle. |
| Posterior view | |
 |
The neck is directed forward and medialward, and
comprises the constricted portion of the bone between the body and the oval
head. Its upper and medial surfaces are rough, for the attachment of ligaments;
its lateral surface is concave and is continuous below with the deep groove for
the interosseous talocalcaneal ligament. The head looks forward and medialward; its anterior articular or navicular surface is large, oval, and convex. Its inferior surface has two facets, which are best seen in the fresh condition. The medial, situated in front of the middle calcaneal facet, is convex, triangular, or semi-oval in shape, and rests on the plantar calcaneonavicular ligament; the lateral, named the anterior calcaneal articular surface, is somewhat flattened, and articulates with the facet on the upper surface of the anterior part of the calcaneus. |
| Anterior view |
Blood supply
It is a common misconception to
consider the blood supply of the talus as poor.
Many vessels, anastomose and form
a rich vascular network all around the talus.
In the narrow areas between the articular surfaces, many strong ligaments are inserted, and on a dry bone many vascular foramina are visible.
The problem is that 2/3 of the bone is covered by cartilage.
 |
 |
 |
|
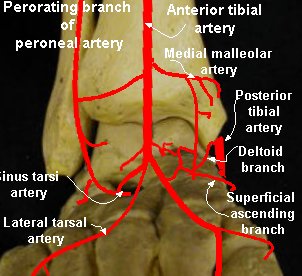
Medial view - blood supply |
Anterior view - blood supply |
Inferior view - blood supply |
The three main arteries of the ankle produce many branches of the vascular
network of the talus.
Posterior tibial artery
The posterior tibial artery gives rise to two important branches, often in a common trunk, 1 cm below the talocrural joint, behind the sustentaculum tali, prior to its division in the calcaneal canal:
The deltoid branch and the tarsal tunnel artery.
-
Deltoid branch - penetrates the deltoid ligament and has some branches entering the bone within the insertion of the deltoid ligament just below the medial malleolar facet.
These branches vascularize the medial part of the body.
-
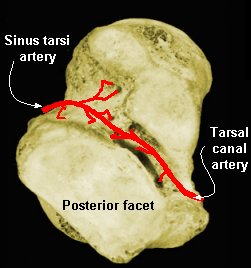
Tarsal canal artery - runs in the tarsal canal ie, the narrow tunnel corresponding to the sulcus tali and the sulcus calcanei. Within this tunnel, this artery runs along the roof, in contact with the bone of the talus to which it is strongly fixed by many penetrating arteries that run upwards and backwards into the bone, providing the main source of blood for the body of the talus.
Since it is firmly fixed on the roof of the tunnel, it is generally preserved in subtalar dislocations.
Below the sustentaculum tali, the medial plantar artery a terminal division of the posterior tibial artery gives rise to a superficial ascending branch to the neck of the talus.
The posterior tibial artery also has some thin branches that form a little thin network for a limited blood supply of the posterior process with some other thin branches of the peroneal artery.
Anterior tibial artery
The anterior tibial artery produces, above the talocrural joint, the anterior malleolar artery and the medial malleolar artery.
Below the talocrural joint, it
becomes the dorsalis pedis artery, which gives rise to many branches over the
neck of the talus forming a rich network that penetrates the bone all
around the head and provides the blood supply to the head.
This network anastomoses on the medial side with the end of the deltoid branch,
with a branch of the
medial malleolar artery, with a branch of the medial plantar artery in front of
the sustentaculum tali, and
with the medial tarsal artery.
On the lateral side of the neck, the dorsalis pedis artery generally forms a main branch for the sinus tarsi network: the sinus tarsi artery.
According to Wildenauer, following the description of Henle, the space between the talus and the calcaneus is like a funnel. The sinus tarsi is the “cone” between the neck, the lateral process of the talus, and the anterior process of the calcaneus. This funnel ends in the canal tarsi (the tube) where the sinus tarsi artery generally anastomoses with the tarsal canal artery.
Perforating branch of the peroneal artery
The sinus tarsi network also anastomoses with the dorsal network of the neck, with the perforating branch of the peroneal artery, with the anterior malleolar lateral artery (in front of the lateral process of the talus) and with the lateral tarsal artery.
Thus, the sinus tarsi network receives branches from the anterior tibial artery (continued dorsalis pedis artery) and from the perforating branch of the peroneal artery.
It vascularizes the lateral process, the anterior part of the body, and the lateral part of the neck.
Classification
Hawkins classification
 |
|
Hawkins sign
|
|
Radiograph 6-8 weeks - subchondral resorbtion good sign. If vascularity of body retained get disuse atrophy and resorbtion of bone. If body retains density suggests avascular, bad sign |

To demonstrate talar neck - place ankle in equinus, place foot on cassette and pronate 15°, x-ray tube is directed cephalad at a 75° from the horizontal.
Treatment
Urgent anatomical reduction needed. If anatomical reduction can treat with cast in slight equinous. MUST be anatomical. Delayed and non union problems due to blood supply.
Weight bearing controversial generally non weight bearing till evidence of healing, may take 2 years.
| Type | Management (Generally) | Duration |
| I | Conservative below knee walking cast (NWB 4-6 wks | 8-12 wks/ x ray healing |
| II | MUA/ ORIF (NWB 8-12 wks may be longer) | > 3mnths/ x ray healing |
| III | ORIF (surgical emergency skin pressure and swelling) | |
| IV | ORIF (As above) |