Weaver Dunn - Arthroscopic
ACJ reconstruction
Indication
Symptomatic Chronic ACJ dislocation
Grade III, IV and V ACJ dislocation
Note: Asymptomatic Grade III ACJ
injury don't require reconstruction
Anatomy
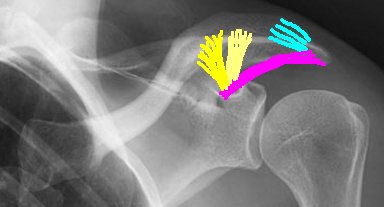 |
Coraco-acromial ligament Acromioclavicular ligaments Coraco-clavicular ligaments |
Considerations
When the ACJ is irreducible total arthroscopic reconstruction is not technically possible, as inability to reduce the clavicle prevents adequate excision of the lateral end of clavicle, requiring open excision.
Positioning
Standard shoulder set up see shoulder arthroscopy positioning
Skin portals
ENSURE THE CLAVICLE IS REDUCIBLE.
4 to 6 portals
1. Standard posterior 2 cm inferior and medial to posterolateral corner of
acromion.
2. Standard lateral 4 cm inferior to lateral acromion.
3. Anterolateral 2 cm anterior and lateral to the anterolateral corner of the
acromion.
4. Posterolateral approximately 2 cm lateral to the posterolateral corner of the
acromion.
5. Anterior to ACJ.
6. Posterior to ACJ.
Except for the standard posterior portal, all portals are made using an “outside in technique.
Procedure
Undertake a routine glenohumeral arthroscopy.
Enter the bursa from the standard posterior portal
Define the lateral border of the Coracoacromial ligament
using a 90°
hook electrode from the anterolateral portal (3.)
Mobilize and define the medial border of the ligament using the anterior ACJ portal (4.)
Using suture passer (Spectrum
corkscrew) pass a 1 PDS suture through the acromial end of the CA ligament,
using the standard lateral (2.) or anterolateral portal (3.)
Repeat the process to creating a whipstitch.
Place a second PDS suture in a similar manner to achieve a firm grasp of the coraco-acromial ligament.
Release the coracoacromial ligament from the acromion.
Park the PDS sutures through the standard lateral portal (2.)
Identify, reduce and arthroscopically excise the lateral end of clavicle. (If clavicle not reducible proceed to open excision).
Via anterolateral portal (3.) to identify and define the coracoid process with a radiofrequency probe without detaching the coracoid insertion of the coraco-acromial ligament, by keeping the probe medial to the insertion.
To protect the ligament transfer till it heals either use a tightrope or suture anchors into the coracoid and sutures around the clavicle to hold the clavicle reduced.
Suture anchor technique.
Place the scope in the anterolateral portal (3.) for improved visualization of the coracoid.
Using the anterior ACJ portal (5.) drill 2 pilot holes in the coracoid (1 anterior and 1 posterior). Insert an anchor into both holes (double thread 5mm with No 2 suture or similar) via the anterior ACJ portal.
Retrieve all 4 sutures from the posterior anchor from the posterior ACJ portal and pass subcutaneoulsly over the clavicle and retrieve them from the anterior ACJ portal.
Effectively creating a loop around the clavicle. Reduce the clavicle and tie the posterior anchor sutures to the anterior anchor sutures.
(Snow et al showed no difference in cerclage versus transosseous tunnels for the clavicle)
Now transfer the coraco-acromial ligament to the clavicle
load an anchor onto each of the PDS sutures previously placed on in the CA ligament. With the camera in the anterolateral portal insert the 2 anchors into the under surface of the distal clavicle and tie the sutures. If the CA ligament is tight release the anterior insertion on the coracoid under direct vision to create more length.
Post operatively
Immobilize in a sling for 6 weeks.
From day 1 perform pendulum and full active assisted ROM.
Avoid heavy lifting and resisting exercises for a further 6 weeks ie. till 3 month post op.
Begin muscular rehabilitation and sports-specific rehabilitation at 3 months
References
Lafosse L, Baier GP, Jan Leuzinger J. Arthroscopic treatment of acute and chronic acromioclavicular joint dislocation. Arthroscopy 2005;21(8):1017
Snow, Martyn MRCS; Funk, Lennard FRCS Technique of Arthroscopic Weaver-Dunn in Chronic Acromioclavicular Joint Dislocation. Techniques in Shoulder & Elbow Surgery. 7(3):155-159, September 2006.