Kocher - Radial head
(Posterolateral approach)
Indication
Radial head excision _+ - replacement
Internal fixation radial head.
Anatomy
See general anatomical considerations about the elbow (link)
Posterior interosseous nerve in supinator.
Pronation moves Posterior
Interosseous Nerve anteriorly and away.
Pronation of the forearm allows safe exposure of at least the proximal 38mm
(measured from capitellum) of the lateral aspect of the radius, with an average
proximal safe zone of 52.0 ± 7.8 mm.
Supination decreases this proximal safe zone to as little as 22mm and an average of 33.4 ± 5.7 mm.
Flexion and extension does not affect the position.
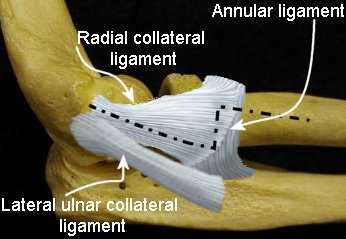 |
During approach, keep deep dissection (dotted line) anterior
to lateral ulnar collateral ligament to prevent posterolateral elbow
instability. Consider Z incision in annular ligament if access to neck required. |
Considerations
For more extensive exposure of elbow consider global approach using Kocher interval
For simple radial head replacement, See Modified posterior approach (Wrightington)
Positioning
Skin incision
Kocher recommended a J shaped skin incision from the lateral supracondylar ridge to the subcutaneous ulna. Alternatives include a posterior midline skin incision and elevation of fasciocutaneous flaps (see global approach)
Superficial dissection
Intermuscular plane - Extensor carpi ulnaris and the anconeus
This interval is visualized as a thin white line along the deep fascia.
Splitting the interval exposes the joint capsule, annular ligament and supinator distally.
Deep dissection
Elevate Extensor carpi ulnaris anteriorly from the lateral collateral ligament complex such that the radial collateral and annular ligaments can be incised at the mid axis of the radial head, thereby staying anterior to the lateral ulnar collateral ligament.
This prevents posterolateral instability of the elbow and allows better exposure of the anterior segments of the radial head that are more commonly injured in patients with radial head fractures.
If greater anterior exposure of the radial head is needed, the radial part of the lateral collateral ligament and common extensor muscle origins can be elevated anteriorly from the lateral epicondyle and supracondylar ridge.
(Kocher recommended that a shell of bone be removed with the lateral epicondyle to preserve the attachment to periosteum, that the lateral capsule be released subperiosteally from the humerus, and that the annular ligament be released from the ulna.)
While rarely required, greater posterior exposure of the radial head can be achieved by elevating the lateral ulnar collateral ligament and the anconeus from its origin on the lateral epicondyle.
Division of the lateral ulnar collateral ligament results in posterolateral rotatory instability of the elbow. Careful repair of this ligament is required to prevent symptomatic instability after internal fixation or replacement of the radial head.
Exposure extension
The exposure can be extended proximally or distally as required to provide greater exposure of the humerus and ulna respectively.
Distal extension
To expose the radial neck:
-
Use a step cut Z incision of the annular ligament anterior to the lateral ulnar collateral ligament. This preserves the lateral ulnar collateral ligament and ensures that the annular ligament can be repaired easily without tension.
-
Split the extensors at their posterior border, identify supinator by its characteristic obliquely oriented fibers, fully pronate the arm to protect the PIN. The supinator is then divided at its posterior border and elevated anteriorly to expose the radial neck.
Proximal extension
See column procedure for use in capsular release.
An extensile lateral exposure is often used for exposure of capitellar fractures
Extend the kocher interval proximally elevating the common extensor origin anteriorly off the supracondylar ridge.
If the lateral epicondyle is fractured mobilize and retract distally the lateral epicondyle including the origins of the common extensors and the lateral collateral ligament.
Elevate any remaining proximal origins of the radial wrist extensor muscles from the lateral supracondylar ridge to improve exposure of the anterior articular fragments. Elevate a triceps-anconeus flap from the posterior aspect of the supracondylar ridge and the olecranon allowing the elbow to dislocate, while hinging on the intact medial collateral ligament. and the proximal part of the olecranon.
With the elbow hinged open it provides exposure of both the anterior and the posterior articular surface of the distal part of the humerus.
Reattach the lateral epicondyle fragment with a lateral plate, suture anchors, trans osseous sutures or fine gauge (22G) figure-of-eight tension-band wire passed through the origin of the common extensor muscle and the lateral osseous column of the humerus.
Ensure a sound repair of the lateral
collateral ligament complex and common extensor origin to prevent posterolateral rotatory instability.
An alternative approach is to divide the common extensor and capsule/ligament
complex as a single layer, in the interval between the extensor carpi radialis
longus and brevis.
The landmarks for this plane are a line joining the lateral epicondyle and
Lister's tubercle.
Closure
Post operatively
Depends on fixation and associated soft tissue injury.
For radial head fractures
-
No significant ligamentous injury: Begin active elbow flexion and extension and forearm rotation immediately, collar and cuff for comfort.
-
Associated ligamentous disruption: Consider a resting splint to protect the soft tissue injury. The forearm is placed in pronation for lateral ligamentous injuries, supination for medial ligamentous injuries, and neutral rotation for combined medial and lateral collateral ligament disruptions.
Avoid passive stretching exercises. (heterotopic ossification)
Strengthening exercises are initiated once there is radiographic evidence of fracture healing, usually by 6-8 weeks after surgery.
References
Diliberti T, Botte MJ, Abrams
RA; Anatomical considerations regarding the posterior interosseous nerve during
posterolateral approaches to the proximal part of the radius.
J Bone Joint Surg Am. 2000 Jun;82(6):809-13.