Anatomical considerations around the elbow
Nerves
Cutaneous nerves
-
Lateral antebrachial cutaneous nerve - At risk during surgery on the lateral aspect of the elbow. It pierces the brachial fascia 3 cm proximal to the lateral epicondyle and passes 4.5 cm medial to the lateral epicondyle. The anterior and posterior branches supply the anterolateral and posterolateral surfaces of the forearm.
-
Medial antebrachial cutaneous nerve - At risk during surgery on the medial aspect of the elbow. The posterior branch divides into two or three branches that cross anywhere from 6 cm proximal to 6 cm distal to the medial epicondyle.
These cutaneous nerves lie just superficial to the deep fascia and are protected if full thickness fasciocutaneous flaps are created. The posterior midline of the elbow has relatively few cutaneous nerves crossing it, and when they do, they usually are small in diameter, as such when possible a midline longitudinal posterior skin incision to minimizes the risk of cutaneous nerve injury.
Radial nerve
The radial nerve courses through the lateral intermuscular septum 10 to 12 cm proximal to the lateral epicondyle. In the anterior compartment, the radial nerve lies between the brachialis and brachioradialis, supplying motor branches to each (only the lateral portion of the brachialis). The radial tunnel is approximately 5 cm long and extends from the level of the radiocapitellar joint to the proximal edge of the superficial head of the supinator muscle. The superficial branch of the radial nerve exits the tunnel proximally, whereas the posterior interosseous nerve diverges posterolaterally to pass beneath the proximal edge of the superficial head of the supinator muscle.
The presence of the posterior interosseous nerve in the substance of the supinator muscle is of paramount importance. When exposing the proximal radius, the posterior interosseous nerve should be protected by stripping the supinator subperiosteally from the radius or ulna (nerve within the muscle), or dividing the superficial humeral head (nerve exposed). With pronation of the forearm, the posterior interosseous nerve is translated approximately 1 cm anteromedially. This concept is important when performing lateral approaches to the elbow, because pronation will increase the zone of safety for the posterior interosseous nerve.
Ulnar nerve
The ulnar nerve passes posteriorly through the medial intermuscular septum and continues distally along the medial margin of the triceps with the superior ulnar collateral artery. The arcade of Struthers is formed by a band of fascia extending from the medial intermuscular septum to the medial head of the triceps and is present in 68% of the population. The ulnar nerve has no branches in the arm. The cubital tunnel is a fibro-osseous tunnel beneath the cubital tunnel retinaculum that bridges the medial epicondyle and olecranon. The ulnar nerve enters the cubital tunnel posterior to the medial epicondyle and grooves the posterior portion of the medial collateral ligament. A few small branches supply the elbow. The ulnar nerve supplies motor branches to the two heads of flexor carpi ulnaris, before passing beneath the arcade of Osborne, or cubital tunnel retinaculum, which is a thickened aponeurotic band bridging the two heads. It then passes between the two heads, to enter the forearm to supply the ulnar half of the flexor digitorum profundus.
Muscles
Triceps brachii
Entire muscle of the posterior compartment of the arm.
-
Long head originates from the infraglenoid tuberosity of the scapula.
-
Lateral head has a linear origin proximal and lateral to the spiral groove, which separates it from the long head.
-
Medial head is deep to the other two heads and originates from below and medial to the spiral groove and widens to include the adjacent intermuscular septae.
Each
head takes origin distal to the other, with progressively larger areas of
origin. The long and lateral heads are superficial and blend in the midline to
form a common superficial tendon, which inserts into the posterior surface of
the proximal olecranon and the adjacent deep fascia. The deep medial head is
fleshy and inserts mainly into the deep surface of the common tendon, with the
remainder inserting into the olecranon and joint capsule, to prevent the capsule
from being "nipped" in extension.
Proximal to the spiral groove, the radial nerve provides branches to the long
and medial heads. Within the spiral groove, branches supply the lateral and
medial heads.
Anconeus
The second branch of the radial nerve to the medial head of triceps traverses it to supply anconeus. This branch is sacrificed during surgical approaches that split the interval between the anconeus and triceps.
Supinator
Supinator lies deep to anconeus and the extensor muscle mass and is important, because of its relationship to the posterior interosseous nerve. The deep ulnar head originates from the crista supinatoris and fossa of the ulna and wraps horizontally around the radius. The superficial humeral head originates from the distal border of the lateral epicondyle, the radial collateral ligament, and the proximal ulna just posterior to the crista supinatoris. The fibres slope downward and overlie the horizontal deep fibres. The arcade of Frohse is the proximal fibrous arch of the superficial head of the supinator muscle. The posterior interosseous nerve innervates both heads and passes between them into the forearm to supply the extensor muscles of the wrist and digits.
Pronator teres
Pronator teres is the most proximal of the flexor pronator group and forms the medial border of the cubital fossa. The large humeral head arises from the medial supracondylar ridge and the anterosuperior aspect of the medial epicondyle. The small ulnar head arises from the coronoid process of the ulna and is absent in 10% of individuals. A fibrous arch connects the two heads and may entrap the median nerve that passes beneath it. The median nerve supplies a branch to each of the heads before it passes between them into the forearm.
Ligaments
The ligamentous complexes that stabilize the joint are thickenings of the capsule on the medial and lateral aspects.
Medial collateral ligament complex
Consists of three components:
-
Anterior bundle - Structurally and biomechanically the most significant component of the medial collateral ligament complex, attaches to the sublime tubercle on the medial aspect of the coronoid process.
-
Posterior bundle - Fan shaped and attaches inferiorly and posteriorly to the axis of rotation on the medial epicondyle. It attaches to the middle of the medial margin of the trochlear notch and is taut during flexion.
-
Transverse bundle - Transverse bundle is not always well-defined and does not significantly contribute to stability.
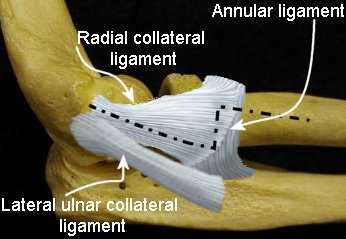
Lateral collateral ligament complex
Consists of three components:
 |
|
References
Clinical orthopaedics and related research; (370), January 2000, pp 19-33; Surgical Approaches to the Elbow; Patterson, Stuart D; Bain, Gregory I; Mehta, Janak A.