Traction
As a general rule for femoral fractures use 10% body weight.
For counter traction elevate bed 5 cm for every 1 Kg (1 inch per 1 lb)
Knots to attach cord to traction device (click here)
Traction types and how to set up traction (click here)
Skin traction
Maximum traction weight 6.7 Kg (15lb), remember skin quality.
Adhesive
Generally for paediatric cases
Non adhesive
For Adult cases, or where thin atrophic skin
If poor quality skin reduce max weight to 4.5Kg (10 lb) or consider skeletal traction.
Skeletal traction
- Steinman pin and Bohler stirrup
- Denham pin, threaded pin engages cortex reducing movement.
- Kirschner wire, on wire tightener
Traction sites
Olecranon
Olecranon
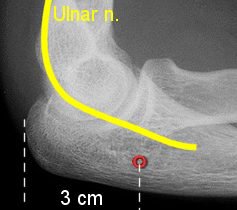 |
K wire from medial to lateral. Right angles to logitudinal axis of ulna 3 cm distal to tip of olecranon Deep to subcutaneous border Avoid ulnar nerve Screw eye can be used directly into tip of Olecranon |
Second and third metacarpals
 |
K wire 2-2.5cm proximal to distal end second metacarpal. Wire traverses the 2nd and 3rd metacarpals transversely To lie at right angles to the longitudinal axis of the radius |
Greater trochanter
 |
Lateral surface of femur 2.5cm below the most prominent part of the greater trochanter Midway between anterior and posterior surfaces of femur
|
Distal femur
Beware knee stiffness, try not use for longer than 2 to 3 weeks
Remember the lateral knee joint capsule reaches 1.25-2cm above knee joint, dont forget the distal femoral physis in children.
In general, the pin should pass along or slightly posterior to the midcoronal plane of the femoral shaft. It should also pass just proximal to the adductor tubercle in order to avoid engagement of the collateral ligaments. This lies almost at the level of the proximal pole of the patella in the relaxed and extended knee.
Flex the knee slightly during insertion to draw the periarticular soft tissues into the position they will occupy while the limb is in traction, thereby reducing pressure necrosis of the skin.
 |
Two methods
|
Proximal tibia
Contraindicated if the knee ligaments have been injured.
Insertion point 2cm distal and posterior to Tibial tuberosity. Dont let the pin creep anteriorly while inserting the pin.
 |
2cm behind and below Tibial tuberosity From Lateral to medial to avoid common peroneal nerve
|
Distal Tibia & Calcaneus
Calcaneal Traction
Ideally, the pin should be inserted as far posterior as
possible while still engaging sound bone. The tendons and neurovascular bundle
passing behind the malleoli and the subtalar joint are to be
avoided.
Halett et al suggests for a calcaneal pin place it 2 cm below and behind the lateral malleolus or 3 cm below and behind the medial malleolus BEWARE Tornetta et al show no position is completely safe when placing a medial calcaneal pin or transcalcaneal pin. Ensure you are as far posterior as possible yet still engaging bone.
 |
|
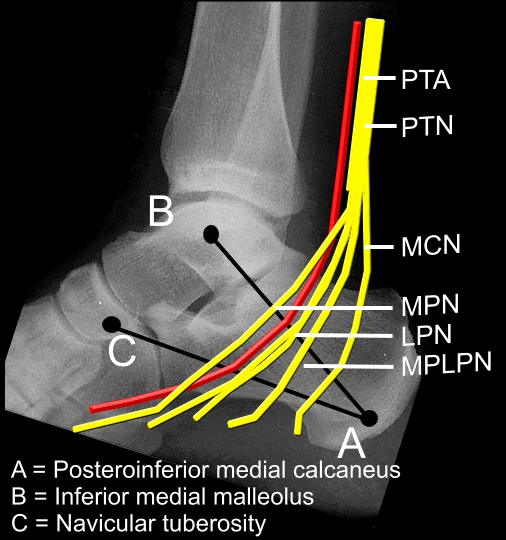 |
The medial calcaneus provides a small window for safe percutaneous
pin placement. A more posterior placement in the safe zone is safest. Careful blunt dissection and the use of cannulas may help to avoid neurovascular injury |
Halo traction
Click here for Halo application
Traction and Orthopaedic Appliances; John D.M Stewart, Jeffrey P. Hallett
Percutaneous pin placement in the medial
calcaneus: is anywhere safe?
Casey D, McConnell T, Parekh S, Tornetta P 3rd.
J Orthop Trauma. 2004 Sep;18(8 Suppl):S39-42.