Scapholunate dissociation
Scapholunate dissociation is the most common carpal instability. Scapholunate instability is associated with increased scaphoid flexion and pronation with associated lunate extension. The abnormal kinematics lead to a decrease in surface area contact at the radioscaphoid joint. This abnormal articulation causes an increased concentration of load, leading to the development of degenerative arthritis. Watson and coworkers described the typical pattern of wrist arthritis related to scapholunate instability, which has been termed scapholunate advanced collapse SLAC wrist. The goals of the surgical reconstructions for a scapholunate dissociation are to relieve the symptoms associated with the instability, maintain motion, and prevent the development of degenerative arthritis.
Acute Scapholunate dissociation
Acute static scapholunate dissociation, which may occur as an isolated entity or as a late sequela of a perilunate dislocation, results from injury to the scapholunate interosseous and palmar radioscaphoid ligaments. Depending on the extent of ligamentous injury, there is either diffuse tenderness of the carpus or point tenderness over the scapholunate interval.
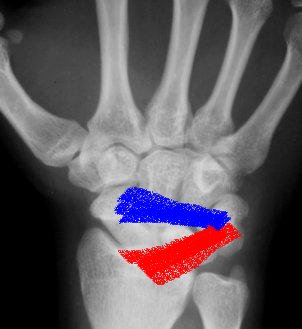
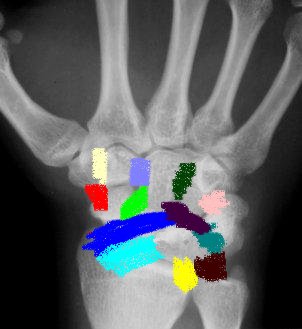
Anatomy
 |
 |
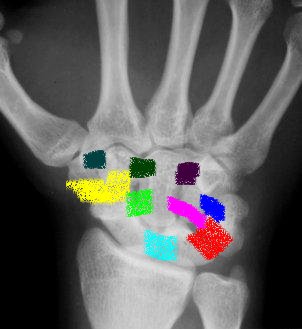 |
| Dorsal extrinsic ligaments | Volar Extrinsic ligaments | Intrinsic ligaments |
Pathology
Which specific ligaments must be injured to cause a scapholunate dissociation is controversial. Several studies have shown that disruption of the scapholunate interosseous ligament changes carpal motion. According to Mayfield, a partial injury of the anterior aspect of the scapholunate interosseous ligament could result in scapholunate instability. Ruby et al. consider the posterior aspect of the scapholunate interosseous ligament as the important mechanical component. Berger et al., on the other hand, suggested that there were no alterations in scaphoid motion with scapholunate interosseous ligament sectioning. Others have proposed that the palmar scaphotrapezoid ligament prevents rotatory subluxation of the scaphoid . Taleisnik noted that the radioscapholunate and radioscaphocapitate ligaments prevent the instability. More recently, Berger and Landsmeer have shown that the radioscapholunate ligament plays less of a role in stabilizing the wrist; its significance may be related to the vascular and neural structures that lie within the ligament. This controversy, as well as the technical difficulties in ligament repair and reconstruction, has led to the numerous procedures described for the treatment of this carpal instability.
Clinical
The patient may give a history of clicking and clunking of the wrist.
On examination, there is tenderness about the scapholunate interval, which lies just distal to the Lister tubercle. Provocative maneuvers for scapholunate instability, such as the scaphoid shift test, may be positive and there is often associated grip strength weakness.
Radiographs
Radiographs reveal key features of rotatory subluxation of the scaphoid.
 Ap view"Terry Thomas"sign gap between scaphoid and lunate normal 1-2 mm (abnormal 3mm) Progressive flexion and foreshortening of the scaphoid leads to the scaphoid ring sign, seeing scaphoid end on. |
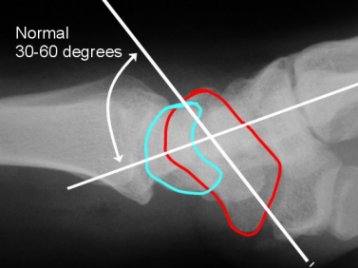 Lateral viewIncreased scapholunate angle normal 30-60º Increased flexion of scaphoid and extension of lunate may progress to DISI (increase capitolunate angle >20º strongly suggestive of carpal instability |
Treatment (acute injuries)
Ligamentous repair within three weeks after the injury is preferred. Delayed repair can be carried out as long as four to six months from the time of the injury.
Neither closed reduction alone nor closed reduction and percutaneous pin fixation is uniformly successful in maintaining carpal alignment and in achieving satisfactory long-term outcomes in wrists with acute scapholunate instability. The preferred method of treatment is open reduction of the carpus through a dorsal approach, pinning of the scaphoid to the lunate and to the capitate with two 1.2mm Kirschner wires, and direct repair of the scapholunate ligament. Ligament repair is carried out either with direct suture for ligaments torn in their midsubstance or with pull-out sutures or suture anchors for ligaments avulsed from bone. The wrist is immobilized in neutral position in an above elbow thumb spica cast for eight weeks, following which time the pins are removed and active motion is initiated
Several factors govern the feasibility of delayed ligamentous repair (repair later than three weeks after the time of the injury):
-
Identification of a substantial, reparable scapholunate interosseous ligament and the isolation of a palmar flexed scaphoid that can be reduced without the necessity for extensive circumferential dissection. The extent to which the scaphoid becomes fixed in palmar flexion is dependent on the magnitude of the initial capsular injury, with scarring and capsular contracture increasing over time.
Chronic Scapholunate Dissociation
For wrists in which the scapholunate interosseous ligament cannot be repaired primarily several reconstructive options exist:
Treatment (chronic)
Reconstructive procedures:
-
Dorsal capsulodesis - Attempts to provide a check rein mechanism to prevent abnormal flexion of the scaphoid.
-
Tendon weaves using free tendon grafts have been performed in the past. These procedures have been abandoned owing to progressive carpal collapse or carpal disintegration caused by the multiple drill holes
-
Scapholunate arthrodesis has been described. There is a high risk of nonunion with the procedure, likely related to the significant forces across this site and the small surface area of the scapholunate interval for fusion.
-
Bone-ligament-bone autografts have been described that are similar in concept to procedures performed for anterior cruciate ligament reconstruction. The graft may be obtained from the dorsal capitohamate interval or the distal radius using a portion of the extensor retinaculum. The foot is an alternative donor site using the dorsal medial portion of the navicular-first cuneiform ligament
Factors affecting choice of reconstruction:
-
Reducibility of the scapholunate interval - a reducible scapholunate interval is required to perform a dorsal capsulodesis. In other words, the procedure is not performed in patients with a fixed dorsal intercalated segment instability carpal collapse deformity.
-
Integrity of the ligament
-
Arthritic change - Dorsal capsulodesis is contraindicated in patients with degenerative changes about the midcarpal or radiocarpal joints. If arthritic changes are evident, one of the salvage procedures should be considered. Preoperative arthroscopy of the wrist can be beneficial in confirming the diagnosis of scapholunate instability and evaluating for degenerative changes about the wrist.
-
Patient-related factors
Salvage procedures
-
Triscaphe arthrodesis is a salvage procedure and is considered if the carpus is not reducible due to the secondary capsular contracture. The procedure is also considered after failure of a soft tissue repair or reconstruction as long as there are no associated degenerative changes about the radiocarpal joint. Intercarpal arthrodesis has been shown to have a greater loss of wrist motion globally compared with dorsal capsulodesis and there is the potential complication of accelerated wear of the radiocarpal joint.
Results
Blatt reported good results in his series of 12 patients treated with dorsal capsulodesis for scapholunate dissociation. His singular criterion for the
procedure was the ability to anatomically reduce the scaphoid at the time of
surgery. He noted a recovery of 80% of grip strength and loss of no more than
20° of wrist flexion.
Wintman et al. retrospectively reviewed 19 patients who had
undergone 20 dorsal capsulodesis for dynamic scapholunate instability. The
diagnosis was based on history of dorsal wrist pain and clunking, tenderness at
the dorsal scapholunate interval, and a positive scaphoid shift test finding.
There was no static instability or arthritic change on radiograph. Mean
postoperative follow-up was 34 months, at which time, overall, patients reported
a decrease in symptoms of pain and clunking as well as improvement of functional
status. The frequency of clunking decreased from less than five times per day
preoperatively to less than once a month postoperatively. Fifteen of 17 patients
returned to their original occupation, although 7 required some restrictions. On
average, there was a 12-degree loss of wrist flexion.
Lavernia et al. combined scapholunate ligament repair with dorsal
capsulodesis in 17 patients and performed a scapholunate ligament repair alone
in 4. The average scapholunate angle was 62° preoperatively and 57° postoperatively. All patients noted decreased pain, although there was
an average loss of wrist flexion of 17°. There was overall patient satisfaction
with the procedure with no progression to advanced collapse in the 3-year
average follow-up period.
In contrast, Wyrick and Kiefhaber reported less than optimal results in
their series of 24 patients who underwent scapholunate ligament repair combined
with dorsal capsulodesis. At an average of 30 months postoperatively, 60% of
their patients still had pain with activities of daily living. In addition, the
ultimate scapholunate angle and gap were not significantly different from
preoperative values. They concluded that the procedure could not be recommended
for static scapholunate instability. Their results may have differed from those
of Lavernia et al. in that the latter study likely included few patients
with true rotatory subluxation of the scaphoid and may have represented more
patients with dynamic instability. It was suggested that repair of the
scapholunate ligament and dorsal capsulodesis be performed with the following
criteria.
-
The repair should be performed in patients less than 1 year from injury.
-
The patient should not perform heavy manual labor.
-
The scapholunate angle should be less than 70°, and the scapholunate gap should be less than 5 mm.
Deshmukh et al. reviewed their experience in treating 44 cases of chronic scapholunate dissociation treated by Blatt capsulodesis. They reported only 24
of 44 (55%) patients with a good or excellent result. There was a decrease in
grip strength and a loss of wrist motion, specifically wrist flexion and radial
deviation. The authors found no statistically significant change in the
scapholunate angle, scapholunate gap or carpal height at follow-up. They noted
several reasons for the less favourable results. There was a long time interval
from injury to surgery, with patients waiting on average 58 months. In addition,
39% of the patients were involved in workers' compensation. They recommended
that the procedure not be performed on a routine basis except in a select group.
The most common complication of the dorsal capsulodesis involves limited wrist
flexion as noted in each of the above described procedures. Dagum et al.
have shown that this loss of wrist flexion is inherently related to the
procedure and not due to scarring after immobilization. Attempts at regaining
the last 12 to 20° of wrist flexion could lead to disruption or weakening of the
reconstruction.
Conclusions
The goal in the treatment of scapholunate dissociation is to stabilize the carpus in the appropriate alignment in addition to maintaining wrist range of motion. The optimal method of attaining these goals is currently controversial. Dorsal capsulodesis is a reconstructive surgical option that acts as a check rein to correct the abnormal alignment of the scaphoid that occurs with scapholunate instability. The procedure does not anatomically reconstruct the scapholunate ligament. It maintains carpal motion but leads to some limitation of wrist flexion. The results of the procedure reported in the literature are conflicting. It appears to provide the best results in patients with less significant static radiographic abnormalities such as in a dynamic instability. Unfortunately, the alternative surgical options are also not ideal, although recent advances in the reconstructive procedures such as the bone-ligament-bone grafts have great potential. At this time, dorsal capsulodesis is a reasonable procedure for dynamic scapholunate instability using appropriate selection criteria.
Dorsal capsulodesis surgical technique (click here)
GILULA, L A; MANN, F A; DOBYNS, J H; YIN, Y; IWIW TERMINOLOGY COMMITTEE WRIST TERMINOLOGY AS DEFINED BY THE INTERNATIONAL WRIST INVESTIGATORS' WORKSHOP (IWIW). Journal of Bone & Joint Surgery - American Volume. 84-A SUPPLEMENT 1:1-66, 2002.
Kaawach, Wael; Ecklund, Kirsten; Di Canzio, James; Zurakowski, David; Waters, Peter M. Normal Ranges of Scapholunate Distance in Children 6 to 14 Years Old. Journal of Pediatric Orthopedics. 21(4):464-467, July/August 2001.
GELBERMAN, RICHARD; COONEY, WILLIAM P. III; SZABO, ROBERT M.; - Carpal Instability. JBJS - A Vol. 82-A(4):578-594, April 2000