Scaphoid fracture
Most common carpal fracture, accounts for 60 to 90% of all osseous wrist injuries. All the blood supply to the proximal part of scaphoid enters at or just distal to the waist. Therefore fractures through the waist or proximal to the waist leave the proximal fragment avascular.
Two different mechanisms of injury have been proposed for scaphoid fractures:
-
Longitudinal compression resulting in a nondisplaced scaphoid fracture
-
Forced hyperextension of the wrist (bending injury) resulting in displacement.
With hyperextension injury to the scaphoid the volar cortex fails in tension and the dorsal cortex of the scaphoid fails in compression.
Anatomy
Gelberman and Menon defined the vascularity of the scaphoid bone as branches off
the radial artery, entering at or distal to the waist of the scaphoid along the
dorsal ridge (the dorsal scaphoid branch). This can account for approximately 70
to 80% of the entire arterial supply to the scaphoid and to 100% of the proximal
pole.
Classification
Scaphoid fractures have been grouped according to time from injury, location,
or
character of fracture. In relation to time, scaphoid fractures can either be (1)
acute fractures - less than 3 weeks from injury, (2) delayed unions - 4 to 6
months out, or (3) nonunions - greater than 6 months from injury. Scaphoid
fractures can also be classified according to location as distal pole, waist,
and proximal pole fractures. Fractures of the waist of the scaphoid are the most
common type. A fracture of the waist or proximal pole of the scaphoid has an
increased incidence of nonunion because of the poor blood supply to these areas.
 |
Classified according to:
|
Healing difficult due to scaphoid's predominantly articular cartilaginous covering and tenuous vascular supply.
Clinical
Suspect a scaphoid fracture in anyone following a fall on the outstretched hand with tenderness in the anatomical snuffbox.
Up to 25% of initial radiographs may not demonstrate a fracture. Obtain scaphoid views if tender in the ASB treat empirically as a scaphopid fracture and obtain further imaging.
Options include:
Repeat radiographs after 10-14 days
Three phase nuclear medicine bone scan
Spiral CT scan
MRI
Radiographs
Standard wrist radiographs PA and lateral are not good enough to exclude a scaphoid fracture.
Malik et al showed that there is very little standardisation among the terminology and views performed under the term "Scaphoid views."
Most radiographers perform 4 views, Malik et al suggest 5 views.
The general principle being the scaphoid is normally flexed and as such ulna deviation elongates the scaphoid, angling the beam or extending the wrist slightly in a PA projection further brings the scaphoid out to length.
The terminology for similar radiographs also differs.
Radiographs and terminology suggested by Malik et al
| Terminology | Anterior oblique | Posterior oblique | lateral | PA in ulnar deviation | PA with ulnar deviation and angled beam 20º |
| Image |
 |
 |
 |
 |
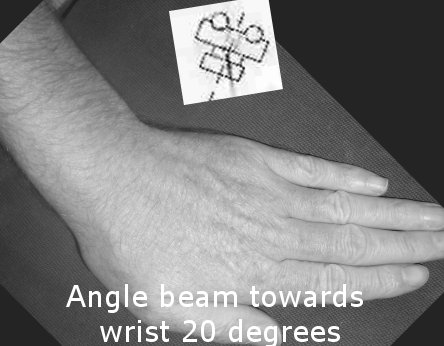 ANGLE
beam 20º ANGLE
beam 20º |
| Alternative descriptions |
Radial oblique Dorsipalmar oblique Semi pronated oblique Oblique pronation 45º oblique PA |
Ulnar oblique Semi supinated oblique 45º oblique AP |
Lateral (navicular) Lateral (scaphoid) |
Ulna deviated PA (UDPA) Navicular view |
Bridgman view Elongated scaphoid "Banana view Ziter view |
| Value | Best for sulcal fractures, waist and tuberosity | Good for proximal pole and dorsal avulsions | Alignment of carpus, tuberosity | Long axis of scaphoid | Very good for waist |
Non operative management
For stable, nondisplaced waist fractures (less than 1 mm displacement), immobilise in cast 9 to 12 weeks, achieves 90 to 100% union when started early.
Remove the cast after 8 to 12 weeks if there is no marked tenderness in the scaphoid region and radiographically the fracture united, (bridging trabeculae on all views of the scaphoid).
Internal fixation
Internal fixation is indicated in:
- Displaced fractures ( >1 mm, radiolunate angle >15º, scapholunate angle >60º)
- Open fractures
- Fractures associated with perilunate dislocations
- Proximal pole fractures (to minimize risk of AVN or non union)
For unstable fractures, the union rate with casting is only 50 to 60%, with those treated late requiring longer immobilization time. The rate of AVN of the proximal pole (50%) parallels that of the nonunion rate for displaced fractures.
Percutaneous screw fixation
Percutaneous fixation is increasingly being advocated for non displaced fractures. It is minimally invasive and reduces the morbidity associated with prolonged cast immobilization. The advantages of percutaneous fixation include high fracture union rate, maintenance of range of motion, and early return to activity or work. Both volar and dorsal percutaneous techniques exist.
Prospective randomized study of nondisplaced mid-waist fractures, Cast versus percutaneous screw fixation.
- Percutaneous screw fixation, fractures healed faster (7.09 vs 11.62 weeks) and the patients returned to work earlier (8.17 vs 15.26 weeks). All fractures united and only one patient required screw removal because of its prominence. Complications from this technique are uncommon, the most worrisome being displacement of the fracture during insertion of the drill or screw due to an oblique angle of approach relative to the fracture orientation.
Open reduction and internal fixation
More controversial is ORIF for stable waist fractures, that is, fractures that should heal with casting in 9 to 12 weeks. However, for working or athletic patients, shorter immobilization after stable fixation offers the advantage of quicker fracture union and thus a faster return to work or sports.
Surgical treatment of unstable fractures (displaced fractures, proximal pole fractures, open fractures, fractures associated with perilunate dislocations) is currently the gold standard, and most, if not all, surgeons recommend ORIF for these fractures to minimize risk of nonunion and AVN.
Proximal pole fractures are at high risk for nonunion and AVN, especially with a greater degree of displacement, because of the tenuous vascular supply to this portion of the scaphoid. If casting is selected as treatment, prolonged immobilization may be required. As such, a majority of surgeons consider this fracture pattern to be an indication for ORIF. A dorsal approach provides the best visualization of the proximal scaphoid.
Scaphoid fixation approaches
Non Union
Nonunion is the most common complication in up to 5% of cases.
Risk factors include
- Delay in diagnosis
- Improper or inadequate immobilization
- Fracture displacement
- Ligamentous instability
- Insufficient blood supply to the proximal pole fragment
References
Charles D. Bond, Alexander Y. Shin, Mark T. McBride, and Khiem D. Dao, Percutaneous Screw Fixation or Cast Immobilization for Nondisplaced Scaphoid Fractures; JBJS - A 2001 83: 483
Sherman, Gary M.; Seitz, William H. Jr; Results: Current Opinion in Orthopedics ; Volume 10(4), August 1999, pp 237-25; Fractures and dislocations of the wrist
A. K. Malik, A. A. Shetty, C. Targett, and J. P.
Compson;Scaphoid views: a need for standardisation. Ann R Coll Surg Engl. 2004
May; 86(3): 165–170.