Acromioclavicular Joint (ACJ)
Acromioclavicular joint injuries are common
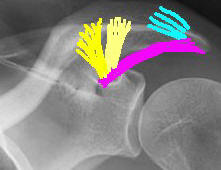
Anatomy
Diarthodial joint
The articular surface of each joint is initially hyaline cartilage, but often
changes to fibrocartilage by 17 to 24 years of age.
|
|
Stability of joint provided by:
|
Mechanism of injury
Direct blow to tip of shoulder with adducted arm
The acromion is driven inferiorly and anteriorly
Classification
Tossy and Allman classified:
-
Type I - AC joint remains well aligned, but the ligaments are strained (or sprained).
-
Type II - Complete rupture of the AC ligaments, and strain of the CC ligaments such that the end of the clavicle is displaced less than 100% of its width.
-
Type III - Both the AC and CC ligaments are ruptured with clavicle displaced more than 100% of its width. In addition, the coracoclavicular interspace is increased by more than 25 to 100%.
Rockwood expanded this classification
|
|
Type I - Sprain of the AC ligaments. Type II - Complete rupture AC ligaments. Type III - Complete rupture AC and CC ligaments. Type IV - Complete rupture AC and CC ligaments. with displacement of clavicle posteriorly through Trapezius Type V - Complete rupture AC and CC ligaments with gross displacement of ACJ and detachment of Deltoid and Trapezius Type VI - Sub coracoid displacement |
Neviaser subdivided type 3 injuries into:
-
III A - ACJ reducible with upward pressure under elbow
-
III B - ACJ not reducible (Neviaser suggested these require operative treatment)
Clinical
Skin integrity, abrasions, tenting
Palpate ACJ and coracoclavicular interspace
Type III and greater have greater deformity
Neurovascular exam of the involved extremity is important
Reducibility of the joint with upward pressure an the elbow stabilizing the the clavicle superiorly (note shoulder drops down, not clavicle moves up)
Radiographs
-
ACJ best seen on direct AP view of shoulder (like CXR), as opposed to scapular AP (the usual AP shoulder(scapular AP) is taken at 30º to the chest perpendicular to plane of the scapula to better visualise the glenohumeral joint)
-
Standard shoulder radiographs overpenetrate the ACJ, reduce voltage by 50%
-
10-15º Caudal tilt eliminates overlap of ACJ on the scapula
-
Stress radiographs may reveal further displacement of the joint but is unlikely to influence treatment therefore not routinely indicated
Management
|
Type I |
|
|
Type II |
|
|
Type III |
|
|
Type IV |
|
|
Type V |
|
|
Type VI |
Nonoperative treatment
Short period of sling support, a few days to a few weeks, and physical therapy
Full activities resumed as comfort allows
Type III injuries
The treatment of type III injuries continues to be a source of debate, several new techniques are being introduced and tried but none have conclusively been shown to be better than non operative treatment.
There is little evidence to support the routine fixation of a grade III ACJ injuries.
Overall 80% of surgically treated and 87% of nonsurgically treated patients had a satisfactory outcome.
Complications are highest among surgically treated patients, occurring in 59% of cases compared with 6% of those treated nonsurgically. Return to activity is no quicker without surgery than following surgery.
Pain was not any more common with surgery than without surgery.
Range of motion was normal in 95% of the nonoperative group compared with 80% of the operated patients and strength recovery was better in the nonoperative patients; 92% compared with 87%.
Perhaps consider surgery in younger individuals who undertake heavy work and overhead athletes.
Operative treatment
Neurovascular structures close by and high forces across the shoulder make surgery technically demanding
Options
-
Simple resection of the distal clavicle (Mumford procedure)- not suitable if greater than type I and II
-
Reduce ACJ +- repair CC ligament reduced using various methods:
-
Bosworth screw - High incidence of failure and technically demanding
-
K wires across ACJ - Migration of K wires around the shoulder
-
Suture/ tape loops around base of coracoid and through clavicle (PDS tape, Ethibond, anchors into coracoid)
-
Artificial ligament reconstruction - (braided polyester "Surgilig")
-
Hook plate
-
Arthroscopic assisted reduction/ reconstruction - "Tightrope"
-
-
Resection of lateral end of clavicle and transfer of the coracoacromial (CA) ligament into the end of the clavicle. Temporary fixation is provided by suture fixation or screw fixation from the clavicle to the coracoid process. (Weaver Dunn - see approaches)
Allman Jr FL: Fractures and ligamentous injuries of the clavicle and its
articulation. J Bone Joint Surg 49A:774-784, 1967.
Tossy JD, Mead MC, Simond HM: Acromioclavicular separations: Useful and
practical classification for treatment. Clin Orthop 28:111-119, 1963.
Acromioclavicular and sternoclavicular injuries in athletes; Rodosky, Mark MD; Jari, Rajesh MD, Current opinion in Orthopaedics: August 2001;12(4) :325-330
Williams GR, Nguyen VD, Rockwood CR. Classification and
radiographic analysis of acromioclavicular dislocations. Appl Radiol
1989;Feb:29–34.
Reconstruction of Chronic and Complete Dislocations
of the Acromioclavicular Joint ;Guy, Daniel K. MD; Wirth, Michael A. MD;
Griffin, James L. MD; Rockwood, Charles A. Jr. MDCurrent Orthopaedics and
related research; February 1998 Vol(347) :138-149