
© Cambridge Fracture Clinic - Mr Lee Van Rensburg - Cambridge; United Kingdom







Metalwork removal
General
A very common question asked in clinic is: "Does the metalwork need to come out?" Plates, screws, wires and metal rods are often used to hold bones together. They get put in to do a job, hold the bones in an optimal position till the bones are healed. There are very few absolute reasons to remove metal work. In general metal is only removed if it is causing or has the potential to cause harm. In all aspects of orthopaedics we are often weighing up the pro's and cons of doing one thing or another. In the 1970's and 80's we were not sure of the long term effect of metal on the body, there were fears of increased risk of tumours and increased risk of late infection. We now know there is no increased risk of tumour or infection around static metal work. It is important this concept of static metal work (plates, screws, nails). In large metal on metal bearing hip replacements the metal wear debris and metal ions may cause problems. Any operation carries with it the potential for complications. You want to be sure the risks of metal work removal justifies the risks. Each case should be judged on its own merits. For example tension band wiring around the point of the elbow is often problematic and tender. It is also easily removed once the fracture has healed and surgery to remove it is associated with a very low complication rate. As such tension band wiring around the elbow is often removed. Plates in the forearm of an adult are very seldom symptomatic and are associated with an up to 20% complication rate when removal is attempted. In high risk individuals (Evil Knieval), people who undertake high risk activities on a daily basis, metal might be removed to prevent a periprosthetic fracture. Where the metal ends becomes a relative stress riser and as such if the limb is subjected to a large stress, the bone often breaks at the end of the metal. This makes treatment more tricky particularly if there is only a small piece of bone left above or below the joint. This was a real problem in the past, with modern surgical techniques and modern implants it is not as much of a problem.Specific metalwork
K- wires (Kirschner wires)
K-wires are stainless steel wires of varying thickness, normally 1-2 mm thick. They are often used for temporary fixation of fractures, most commonly around the wrist. They are often left proud of the skin and as such can be pulled out in clinic. K-wires that need to be in place for more than 6 weeks may be buried under the skin, requiring surgery to open the skin and allow removal.Hook Plate
The hook plate is inserted into the shoulder to hold the lateral clavicle in a good position. It is used in some fractures of the lateral clavicle and some dislocations of the Acromioclavicular join (ACJ). The hook plate is generally considered a temporary device. It is only not removed in exceptional circumstances. The reason the hook plate is removed, is because it may cause symptoms of shoulder impingement and problems with the shoulder rotator cuff. With time it may also erode the under surface of the acromion, weakening it and predisposing the acromion to fracture.Intramedullary Nails
In general intramedullary nails are not removed unless you are Evil Knieval and undertake risky activities on a daily basis. An intramedullary nail is stiffer than normal bone and as such patients often get a little aching and discomfort when stressing the limb. Removal may improve this but not totally remove the aching of a previously broken bone. In patients who have had a tibial nail, pain under the knee cap in the front of the knee is common. This may be improved in 50%of cases with removal of the nail, but complete resolution of symptoms is not guaranteed. A relative indication might be the future need for a joint replacement.Risks of surgery
All surgery is associated with varied risks and potential complications. The general risks of metalwork removal include: Anaesthetic Except for percutaneous k-wire wires, metalwork removal is generally undertaken under a light general anaesthetic Infection The infection rate for elective metal work removal is less than 1:100 Inability to remove the metal This is unusual but a real problem. In modern plates and nails, the screws sometimes have threaded heads that lock into the plate. The screw and the plate can cold weld together making removal difficult. Screw heads can strip and on occasion the head may shear off the screw. When it comes to nail removal the insertion and removal thread may become damaged or stripped. There are several techniques to remove broken screws and deal with stripped threads, however on occasion the surgery to remove the metal may be causing more harm than good and as such metal work removal may be abandoned. Neurovascular injury Neurovascular injury, the nerves and blood vessels often follow a predictable path. Following trauma and surgery it can be difficult sometimes to find the nerves and the blood vessels. The deeper the metal work and the nearer it is to the path of the major nerves and blood vessels the higher the risk of injury. Refracture When the metal work is removed it leaves the bone a little vulnerable for around six weeks, till the screw holes have filled in and the bone had a chance to remodel and increase its strength.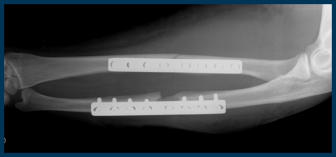






© Cambridge Fracture Clinic - Mr Lee Van Rensburg -
Cambridge; United Kingdom






Metalwork removal
General
A very common question asked in clinic is: "Does the metalwork need to come out?" Plates, screws, wires and metal rods are often used to hold bones together. They get put in to do a job, hold the bones in an optimal position till the bones are healed. There are very few absolute reasons to remove metal work. In general metal is only removed if it is causing or has the potential to cause harm. In all aspects of orthopaedics we are often weighing up the pro's and cons of doing one thing or another. In the 1970's and 80's we were not sure of the long term effect of metal on the body, there were fears of increased risk of tumours and increased risk of late infection. We now know there is no increased risk of tumour or infection around static metal work. It is important this concept of static metal work (plates, screws, nails). In large metal on metal bearing hip replacements the metal wear debris and metal ions may cause problems. Any operation carries with it the potential for complications. You want to be sure the risks of metal work removal justifies the risks. Each case should be judged on its own merits. For example tension band wiring around the point of the elbow is often problematic and tender. It is also easily removed once the fracture has healed and surgery to remove it is associated with a very low complication rate. As such tension band wiring around the elbow is often removed. Plates in the forearm of an adult are very seldom symptomatic and are associated with an up to 20% complication rate when removal is attempted. In high risk individuals (Evil Knieval), people who undertake high risk activities on a daily basis, metal might be removed to prevent a periprosthetic fracture. Where the metal ends becomes a relative stress riser and as such if the limb is subjected to a large stress, the bone often breaks at the end of the metal. This makes treatment more tricky particularly if there is only a small piece of bone left above or below the joint. This was a real problem in the past, with modern surgical techniques and modern implants it is not as much of a problem.Specific metalwork
K- wires (Kirschner wires)
K-wires are stainless steel wires of varying thickness, normally 1-2 mm thick. They are often used for temporary fixation of fractures, most commonly around the wrist. They are often left proud of the skin and as such can be pulled out in clinic. K-wires that need to be in place for more than 6 weeks may be buried under the skin, requiring surgery to open the skin and allow removal.Hook Plate
The hook plate is inserted into the shoulder to hold the lateral clavicle in a good position. It is used in some fractures of the lateral clavicle and some dislocations of the Acromioclavicular join (ACJ). The hook plate is generally considered a temporary device. It is only not removed in exceptional circumstances. The reason the hook plate is removed, is because it may cause symptoms of shoulder impingement and problems with the shoulder rotator cuff. With time it may also erode the under surface of the acromion, weakening it and predisposing the acromion to fracture.Intramedullary Nails
In general intramedullary nails are not removed unless you are Evil Knieval and undertake risky activities on a daily basis. An intramedullary nail is stiffer than normal bone and as such patients often get a little aching and discomfort when stressing the limb. Removal may improve this but not totally remove the aching of a previously broken bone. In patients who have had a tibial nail, pain under the knee cap in the front of the knee is common. This may be improved in 50%of cases with removal of the nail, but complete resolution of symptoms is not guaranteed. A relative indication might be the future need for a joint replacement.Risks of surgery
All surgery is associated with varied risks and potential complications. The general risks of metalwork removal include: Anaesthetic Except for percutaneous k-wire wires, metalwork removal is generally undertaken under a light general anaesthetic Infection The infection rate for elective metal work removal is less than 1:100 Inability to remove the metal This is unusual but a real problem. In modern plates and nails, the screws sometimes have threaded heads that lock into the plate. The screw and the plate can cold weld together making removal difficult. Screw heads can strip and on occasion the head may shear off the screw. When it comes to nail removal the insertion and removal thread may become damaged or stripped. There are several techniques to remove broken screws and deal with stripped threads, however on occasion the surgery to remove the metal may be causing more harm than good and as such metal work removal may be abandoned. Neurovascular injury Neurovascular injury, the nerves and blood vessels often follow a predictable path. Following trauma and surgery it can be difficult sometimes to find the nerves and the blood vessels. The deeper the metal work and the nearer it is to the path of the major nerves and blood vessels the higher the risk of injury. Refracture When the metal work is removed it leaves the bone a little vulnerable for around six weeks, till the screw holes have filled in and the bone had a chance to remodel and increase its strength.


