© Cambridge Fracture Clinic - Mr Lee Van Rensburg - Cambridge; United Kingdom







Clavicle Fractures
General
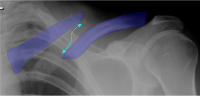
Clavicle (Collar bone) fractures are very common in the young and old. For clavicle fractures in children. (see below) The clavicle connects the arm and shoulder to the rest of the body. In general treatment, outcome and prognosis depends on where along the clavicle it is broken. In the middle third, lateral third, or medial third. The middle third being the most common then lateral and rarely the medial third. Speed of healing varies depending on age, displacement of fracture fragments, degree of comminution and where it is broken (Middle, medial, lateral). Displaced fracture middle third of clavicle, if you cant see it mouse over the image. Note shortening of fracture.Diagnosis
The diagnosis of clavicle fractures is usually straightforward, the tender bump is visible and patients often feel the bones clicking and moving under the skin. An X ray will often confirm or exclude a fracture. Sometimes it is difficult to see exactly how the fracture fragments are aligned and further x ray views may be requested. CT scans may be needed if a fracture is being slow to heal, to see if it is definitely healed or not. CT scans are rarely needed for a simple fracture only sometimes in medial third fractures.Treatment
Treatment depends predominantly on the site: • Middle third • Lateral third • Medial thirdMiddle third (treatment)
Middle third fractures are the most common. Non operative treatment remains the predominant treatment option, particularly in children and in adults with undisplaced fractures. Operative treatment (surgery) may be offered if the fracture is comminuted, displaced or significantly shortened (1.5 to 2cm). Non Operative treatment (middle third) Treatment is purely symptomatic. A little movement stimulates healing, too much movement slows it down. A broad arm sling is used to support the arm for comfort. Use the arm for the activities of daily living, lifting nothing much heavier than a cup of tea for six weeks. This is then followed by a gradual increase in activities both in intensity and duration. The clicking and movement of the fracture gradually reduces as the bones begin to become sticky and set. "Listen" to the fracture, not literally but figuratively. If it aches a little that is OK, if it really hurts and aches that night or the next day after increased activity you have done a little too much. That does not mean stop completely, just come down a little on your activities followed by a graduated increase in activity. Figure of eight bandages have been used in the past in an attempt to splint out the clavicle to length. They make absolutely no difference and although in some parts of Europe they are still used they are of no value. Operative treatment (middle third) The only real absolute indication for an early operation in a clavicle fracture is in an open fracture. In adults if the bone ends are separated (displaced) and or broken into a number of little pieces (comminuted) it may take a long time to heal and some will not heal fully by 6 months. If the bone ends overlap and are shortened by 1.5 to 2 cm, you may notice some fatigability of the shoulder and shoulder function will not be as good as before the fracture. Not desperate but noticeable if you have high functional demands on the shoulder. It is possible to operate at any time if the fracture does not heal fully and achieve bony healing. BUT There is something to be said for having an operation early on to allow for early return to function and optimizing function, particularly in a world that moves very quickly. DOWNSIDE No operation is without risk. Although patients with a comminuted, displaced fractured treated with an operation will have better shoulder function and return to normal activity faster than with non operative treatment. No operation is without risk complications of surgery: • Anaesthetic • Infection/ Local wound healing problem • Tender scar • Nerve injury - particularly the small nerves over the front of the chest below the scar • Blood vessel injury - This is rare but serious, there is a reported deat from injury to the vessels behind the collar bone. • Prominent plate - and possible need for future removal • Persistent Non union - risk is less for post surgery but not zero Methods of fixation: There are several ways of fixing a clavicle, broadly grouped into two methods: 1. Plate and screw fixation 2. Intramedullary screw or nail fixation In essence the plate and screw fixation is more secure and allows for earlier return to heavy duty overhead activity, the down side being a bigger scar and the prominent plate that sits just under the skin. Intramedullary screw or nail fixation is not as strong, but still realigns the bones improving healing times. The smaller scar and absence of prominent plate and screws may be more appealing. Sometimes the screw head or TENS nail may be prominent and need removal.Lateral third
Treatment of lateral third fractures depends largely on whether the fracture fragments are displaced or undisplaced. Most undisplaced fractures are treated non operatively. Non operative treatment of lateral third fractures As for treatment of mid third clavicle fractures (see above) Operative treatment of lateral third clavicle fractures If the fracture fragments are displaced they take longer to heal and will only heal in 2/3rds of cases. In 1/3rd of cases it will not heal with bone but scar tissue and go on to a fibrous non union. Elderly patients with low functional demands will tolerate a fibrous non union. Younger patients with higher functional demands might be symptomatic and need fixation at a later date. An option exists to fix it from the outset to speed up recovery and optimise function. It does depend a little on the fracture configuration as to how easy it is to fix. Surgical options 1. Plate and screw fixation; standard plate, hook plate 2. Suture fixation; tightrope. The potential complications of operative treatment of middle and lateral third fractures are the same. (click here)Medial third
Fractures of the medial third of the clavicle are rare. The pull of the muscles often displaces the fracture fragments. Treatment is very much individualized on the patients needs, fracture configuration and ability or not as it happens to reduce and fix the fracture.Clavicle Fractures in Children
Clavicle fractures in children most often involve the middle third of the clavicle over 90% of these will heal with non operative treatment with very little functional deficit. There is a slight grey zone in adolescents when there is a lot of shortening of the fracture, (over 1.5 to 2 cm).References
Andersen K, Jensen PO, Lauritzen J. Treatment of clavicular fractures. Figure of eight bandage versus a simple sling. Acta Orthop Scand. 1987;58:71-4. "Seventy-nine out-patients with midclavicular fractures were included in a prospective, randomized trial comparing treatment with a figure-of-eight bandage and a simple sling. Sixty-one patients completed the study and were reevaluated clinically and radiographically after 3 months. We found that treatment with a simple sling caused less discomfort and perhaps fewer complications than with the figure-of-eight bandage. The functional and cosmetic results of the two methods of treatment were identical and alignment of the healed fractures was unchanged from the initial displacement.”






© Cambridge Fracture Clinic - Mr Lee Van Rensburg -
Cambridge; United Kingdom






Clavicle Fractures
General
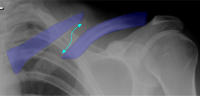
Clavicle (Collar bone) fractures are very common in the young and old. For clavicle fractures in children. (see below) The clavicle connects the arm and shoulder to the rest of the body. In general treatment, outcome and prognosis depends on where along the clavicle it is broken. In the middle third, lateral third, or medial third. The middle third being the most common then lateral and rarely the medial third. Speed of healing varies depending on age, displacement of fracture fragments, degree of comminution and where it is broken (Middle, medial, lateral). Displaced fracture middle third of clavicle,Diagnosis
The diagnosis of clavicle fractures is usually straightforward, the tender bump is visible and patients often feel the bones clicking and moving under the skin. An X ray will often confirm or exclude a fracture. Sometimes it is difficult to see exactly how the fracture fragments are aligned and further x ray views may be requested. CT scans may be needed if a fracture is being slow to heal, to see if it is definitely healed or not. CT scans are rarely needed for a simple fracture only sometimes in medial third fractures.Treatment
Treatment depends predominantly on the site: • Middle third • Lateral third • Medial thirdMiddle third (treatment)
Middle third fractures are the most common. Non operative treatment remains the predominant treatment option, particularly in children and in adults with undisplaced fractures. Operative treatment (surgery) may be offered if the fracture is comminuted, displaced or significantly shortened (1.5 to 2cm). Non Operative treatment (middle third) Treatment is purely symptomatic. A little movement stimulates healing, too much movement slows it down. A broad arm sling is used to support the arm for comfort. Use the arm for the activities of daily living, lifting nothing much heavier than a cup of tea for six weeks. This is then followed by a gradual increase in activities both in intensity and duration. The clicking and movement of the fracture gradually reduces as the bones begin to become sticky and set. "Listen" to the fracture, not literally but figuratively. If it aches a little that is OK, if it really hurts and aches that night or the next day after increased activity you have done a little too much. That does not mean stop completely, just come down a little on your activities followed by a graduated increase in activity. Figure of eight bandages have been used in the past in an attempt to splint out the clavicle to length. They make absolutely no difference and although in some parts of Europe they are still used they are of no value. Operative treatment (middle third) The only real absolute indication for an early operation in a clavicle fracture is in an open fracture. In adults if the bone ends are separated (displaced) and or broken into a number of little pieces (comminuted) it may take a long time to heal and some will not heal fully by 6 months. If the bone ends overlap and are shortened by 1.5 to 2 cm, you may notice some fatigability of the shoulder and shoulder function will not be as good as before the fracture. Not desperate but noticeable if you have high functional demands on the shoulder. It is possible to operate at any time if the fracture does not heal fully and achieve bony healing. BUT There is something to be said for having an operation early on to allow for early return to function and optimizing function, particularly in a world that moves very quickly. DOWNSIDE No operation is without risk. Although patients with a comminuted, displaced fractured treated with an operation will have better shoulder function and return to normal activity faster than with non operative treatment. No operation is without risk complications of surgery: • Anaesthetic • Infection/ Local wound healing problem • Tender scar • Nerve injury - particularly the small nerves over the front of the chest below the scar • Blood vessel injury - This is rare but serious, there is a reported deat from injury to the vessels behind the collar bone. • Prominent plate - and possible need for future removal • Persistent Non union - risk is less for post surgery but not zero Methods of fixation: There are several ways of fixing a clavicle, broadly grouped into two methods: 1. Plate and screw fixation 2. Intramedullary screw or nail fixation In essence the plate and screw fixation is more secure and allows for earlier return to heavy duty overhead activity, the down side being a bigger scar and the prominent plate that sits just under the skin. Intramedullary screw or nail fixation is not as strong, but still realigns the bones improving healing times. The smaller scar and absence of prominent plate and screws may be more appealing. Sometimes the screw head or TENS nail may be prominent and need removal.Lateral third
Treatment of lateral third fractures depends largely on whether the fracture fragments are displaced or undisplaced. Most undisplaced fractures are treated non operatively. Non operative treatment of lateral third fractures As for treatment of mid third clavicle fractures (see above) Operative treatment of lateral third clavicle fractures If the fracture fragments are displaced they take longer to heal and will only heal in 2/3rds of cases. In 1/3rd of cases it will not heal with bone but scar tissue and go on to a fibrous non union. Elderly patients with low functional demands will tolerate a fibrous non union. Younger patients with higher functional demands might be symptomatic and need fixation at a later date. An option exists to fix it from the outset to speed up recovery and optimise function. It does depend a little on the fracture configuration as to how easy it is to fix. Surgical options 1. Plate and screw fixation; standard plate, hook plate 2. Suture fixation; tightrope. The potential complications of operative treatment of middle and lateral third fractures are the same. (click here)Medial third
Fractures of the medial third of the clavicle are rare. The pull of the muscles often displaces the fracture fragments. Treatment is very much individualized on the patients needs, fracture configuration and ability or not as it happens to reduce and fix the fracture.Clavicle Fractures in Children
Clavicle fractures in children most often involve the middle third of the clavicle over 90% of these will heal with non operative treatment with very little functional deficit. There is a slight grey zone in adolescents when there is a lot of shortening of the fracture, (over 1.5 to 2 cm).References
Andersen K, Jensen PO, Lauritzen J. Treatment of clavicular fractures. Figure of eight bandage versus a simple sling. Acta Orthop Scand. 1987;58:71-4. "Seventy-nine out-patients with midclavicular fractures were included in a prospective, randomized trial comparing treatment with a figure- of-eight bandage and a simple sling. Sixty-one patients completed the study and were reevaluated clinically and radiographically after 3 months. We found that treatment with a simple sling caused less discomfort and perhaps fewer complications than with the figure-of-eight bandage. The functional and cosmetic results of the two methods of treatment were identical and alignment of the healed fractures was unchanged from the initial displacement.”