© Cambridge Fracture Clinic - Mr Lee Van Rensburg - Cambridge; United Kingdom







Acromioclavicular joint injuries
General
The Acromioclavicular joint (ACJ) is the joint on the top of your shoulder. It is the joint where your clavicle (collar bone) joins your acromion (part of scapula/ shoulder blade). The ACJ is injured by falling on the point of the shoulder and is a very common injury. It may be referred to as a dislocation of the ACJ, this is not to be confused with a true dislocation of the shoulder. In some countries it is referred to as a shoulder separation. The joint dislocates because the ligaments that stabilise the ACJ and the clavicle get torn to a varying degree. It is the severity of this ligamentous/ soft tissue injury that dictates the treatment options. ACJ injuries are commonly graded 1 to 6. The higher the grade the more severe the injury and the more likely surgery will be needed to obtain a good result.Anatomy
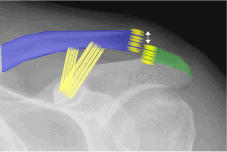
The Clavicle joins the Acromion at the ACJ and is stabilized by the acromioclavicular ligaments (ACJ) and the coracoclavicular ligaments (CC) Mouseover for normal x ray The clavicle is held in place by two sets of ligaments. The ACJ ligaments and the coracoclavicular (CC) ligaments. The ACJ ligaments connect the clavicle and the acromion. The CC ligaments (coracoclavicular) ligaments connect the coracoid to the clavicle and help hold it down.Diagnosis
The diagnosis is usually made on the history of the patient falling directly on the point of the shoulder. Pain is felt mostly on the top of the shoulder. Depending on the severity of the injury a bump may be noticeable from the prominent clavicle (collar bone). In minor injuries grade 1 and 2 the x- rays may be normal or nearly normal. If all the ligaments have been injured then the collar bone will be out of alignment usually gone upwards, sometimes backwards and very rarely downwards. Grade 2 ACJ injury Note clavicle only slightly elevated with rupture of ACJ ligaments. The CC ligaments are still intact. Mouse over for unenhanced x ray Grade 5 ACJ injury Note how high the end of the clavicle is elevated. The ACJ and CC ligaments have completely ruptured and the end of the clavicle has ruptured through the trapezial fascia. Mouse over for unenhanced x ray Stress radiographs are sometimes requested although rarely do they alter the final treatment and prognosis.Treatment
Treatment depends on the severity of the injury and how displaced the clavicle is. In grade 1 and 2 injuries where the Coracoclavicular (CC) ligaments remain intact treatment is non operative. Treatment of grade 3 injuries remains controversial. The main reason it remains controversial is as the bump and deformity is striking, shoulder and arm function is usually very good with non operative treatment. Patients will often get back to work and sport faster with non operative treatment of grade 3 ACJ injuries. Similarly no operation is without the potential for complications. Around 10% of people with grade 3 injuries treated with non operative treatment will have persistent problems with the upper limb and good reconstructive options remain if not healing well eg.(modified weaver Dunn). The only thing you lose with non operative treatment is time. Surgery is not the perfect solution for grade 3 ACJ injuries either, around 10% of operatively treated grade 3 injuries will have some form of problem. (See operative treatment) Grade 4 and 5 injuries are less likely to settle with non operative treatment and as such surgery might be a better option early on. Having said that, it is still possible to treat it non operatively in the first instance. The bump/ deformity will never disappear but it is surprising what good function can be achieved with non operative treatment. It is always possible to do a later reconstructive procedure if the arm function is not satisfactory. The problem with the higher grade injuries is less people will do well with non operative treatment and as such on balance in some cases, if time is of the essence and high level overhead shoulder function is needed, it may be better to operate early. Several variables need to be considered when treating these injuries (See operative treatment) Grade 6 injuries are extremely rare and require surgical treatment.Non operative treatment
Non operative treatment involves relative rest, analgesia and sensible use of the arm till the ligaments heal. Relative rest - muscle ligaments and bones like a little movement while healing and will ultimately heal stronger if gently stressed while healing. However if you keep overdoing it, it will slow the healing process down. Listen to your shoulder, not literally but figuratively - "If it hurts you are doing too much, if not you are doing too little. Don't do nothing , keep the range of motion in your shoulder gently stretch it a few times a day. Use a broad arm sling to support the arm when aching and to stop you from swatting a fly and grabbing a falling cup. Discard the sling as the shoulder settles and pain reduces. Ligaments take time to heal, around 4-8 weeks.Operative treatment
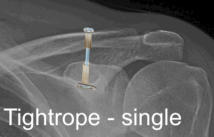
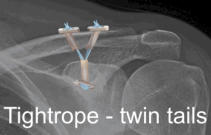
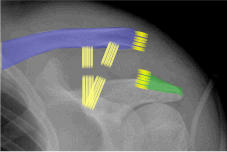
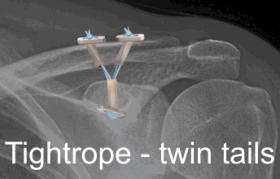
Several options have been tried to solve the problem of ACJ dislocation, some listed below: K - Wires Bosworth screw Hook plate Nottingham sling (Surgilig) Tightrope (open and all arthroscopic, 2 strand twin tails) Artificial ligaments (Lars ligament) Ligament reconstruction (Hamstring autograft) K wires Of all the surgical options this method is not advisable. Although it is possible to simply reduce the collar bone down to the acromion and then pass wires percutaneously through the skin. This method is not secure enough and the complication rate includes migration of the wires. Bosworth screw In an attempt to obtain more secure fixation, a screw is placed through the clavicle into the coracoid. The problem with this is, elevation of the arm above shoulder height induces a rotational force on the clavicle which would lead to loosening and fatigue failure of the screw. A drill hole into the base of the coracoid also weakens the coracoid and could lead to coracoid fracture. A coracoid fracture is very difficult to deal with Hook plate The hook plate is a very powerful way of holding the clavicle reduced to the correct level alongside the acromion. The problem with the hook plate is it requires removal at a later date as the hook under the acromion can cause problems with the tendons of the shoulder and with time can erode through the bone of the acromion. Hence it means 2 operations, one to insert and one to remove. The hook under the acromion may also limit arm movement above shoulder height till it is removed. The timing of removal is around 3 months following insertion. The clavicle may pop back up after removal if removed prior to sound ligament healing. Nottingham sling (Surgilig/ lockdown) In this procedure a synthetic ligament is looped around the coracoid and over the clavicle, holding the clavicle reduced to the level of the acromion. It is very effective and strong avoiding the problems of the hook plate. This strong construct may also create problems. In one of the original series of 11 patients, there was a coracoid fracture. (See references) Coracoid fractures are not easy to deal with. With such a strong permanent structure any further trauma to the shoulder must dissipate through the coracoid or the clavicle. Tightrope/ twin tails It is possible to reconstruct the coracoclavicular ligaments with synthetic suture material (fibrewire). It is possible to insert this in an all arthroscopic way or open. A hole is drilled in the clavicle and coracoid base and the fibrewire passed through the holes. The fibrewire is secured under the coracoid and above the clavicle with a button. Although it is possible to do this all arthroscopically and with small incisions, it is a technically demanding procedure. It requires drilling a hole in the base of the coracoid. This weakens the coracoid and if multiple passes are used with the guide wire or the coracoid is drilled eccentrically it can significantly weaken the coracoid. The single strand construct may also fatigue fail, hence the double strand construct was devised. This also replicates normal anatomy, the CC ligament composed of two distinct strands. Although this is mechanically much stronger the risk of coracoid fracture remains. A coracoid fracture although rare is difficult to deal with. The larger the hole in the base of the coracoid the greater the risk of fracture. Artificial ligament Very similar to the nottingham sling or surgilig there are different artificial synthetic ligaments to reconstruct the coracoclavicular ligament eg Lars ligament. These are very strong and loop around the under surface of the coracoid, the risk remains with the rigid construct of coracoid fracture. Ligament reconstruction (hamstring autograft) It is possible to reconstruct the coracoclavicular ligaments with natural tendons, either from a donor (allograft) or from your own body (autograft). Very similar to the way the anterior cruciate ligament in the knee is reconstructed. This biological reconstruction is less rigid than the artificial ligaments, but carries all the risks and problems of tendon grafts. Where the tendon is attached to the bone is also through bone tunnels, these are weak points in the coracoid and clavicle and could lead to fractures later on. In summary there are several surgical options available none perfect for everyone, each with there own pro's and con's. Treatment whether non operative or operative is very much an individual decision based on the severity of the injury and the patients expectations and needs.Outcome
The outcome is very variable, most grade 1 and 2 injuries settle with non operative treatment. Most Grade 3 injuries settle with non operative treatment, and those that don't it is still possible to undertake reconstruction at a later date with a modified weaver dunn procedure. In grade 4 and 5 injuries the outcome is more variable and often early surgery is advisable.References
Chronic acromioclavicular separation: the medium term results of coracoclavicular ligament reconstruction using braided polyester prosthetic ligament. Jeon IH, Dewnany G, Hartley R, Neumann L, Wallace WA. Injury. 2007 Nov;38(11):1247-53 In this series, we treated chronic acromioclavicular disruption with an artificial coraco-clavicular ligament made from braided polyester (The Nottingham Surgilig). The ligament has a loop at each end and is passed around the coracoid process, threaded through itself, then passed around the posterior aspect of the clavicle and finally anchored to it with a bone screw. Eleven men with an average age of 39 underwent this procedure. Three patients had previously been operated on using the Weaver—Dunn procedure which had failed. All eleven patients have been reassessed clinically and radiographically at an average of 55 months. Using the Imatani evaluation score, 10 patients achieved a good/ excellent result with the mean Constant score being 92. One patient had fracture of the base of the coracoid after heavy lifting in the early postoperative period which resulted in a poor outcome. Two patients needed an additional operation. In one the lateral end of the clavicle was excised together with removal of the fixation screw, and in the other a subacromial decompression was carried out. The Nottingham Surgilig is a useful alternative for the treatment of chronic acromioclavicular separation, especially in revision reconstruction when the coracoacromial ligament is no longer available.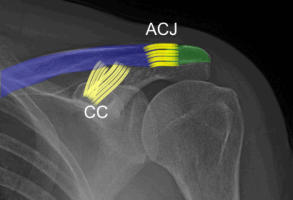














© Cambridge Fracture Clinic - Mr Lee Van Rensburg -
Cambridge; United Kingdom






Acromioclavicular
joint injuries
General
The Acromioclavicular joint (ACJ) is the joint on the top of your shoulder. It is the joint where your clavicle (collar bone) joins your acromion (part of scapula/ shoulder blade). The ACJ is injured by falling on the point of the shoulder and is a very common injury. It may be referred to as a dislocation of the ACJ, this is not to be confused with a true dislocation of the shoulder. In some countries it is referred to as a shoulder separation. The joint dislocates because the ligaments that stabilise the ACJ and the clavicle get torn to a varying degree. It is the severity of this ligamentous/ soft tissue injury that dictates the treatment options. ACJ injuries are commonly graded 1 to 6. The higher the grade the more severe the injury and the more likely surgery will be needed to obtain a good result.Anatomy
The Clavicle joins the Acromion at the ACJ and is stabilized by the acromioclavicular ligaments (ACJ) and the coracoclavicular ligaments (CC) The clavicle is held in place by two sets of ligaments. The ACJ ligaments and the coracoclavicular (CC) ligaments. The ACJ ligaments connect the clavicle and the acromion. The CC ligaments (coracoclavicular) ligaments connect the coracoid to the clavicle and help hold it down.Diagnosis
The diagnosis is usually made on the history of the patient falling directly on the point of the shoulder. Pain is felt mostly on the top of the shoulder. Depending on the severity of the injury a bump may be noticeable from the prominent clavicle (collar bone). In minor injuries grade 1 and 2 the x-rays may be normal or nearly normal. If all the ligaments have been injured then the collar bone will be out of alignment usually gone upwards, sometimes backwards and very rarely downwards. Grade 2 ACJ injury Note clavicle only slightly elevated with rupture of ACJ ligaments. The CC ligaments are still intact. Grade 5 ACJ injury Note how high the end of the clavicle is elevated. The ACJ and CC ligaments have completely ruptured and the end of the clavicle has ruptured through the trapezial fascia. Stress radiographs are sometimes requested although rarely do they alter the final treatment and prognosis.Treatment
Treatment depends on the severity of the injury and how displaced the clavicle is. In grade 1 and 2 injuries where the Coracoclavicular (CC) ligaments remain intact treatment is non operative. Treatment of grade 3 injuries remains controversial. The main reason it remains controversial is as the bump and deformity is striking, shoulder and arm function is usually very good with non operative treatment. Patients will often get back to work and sport faster with non operative treatment of grade 3 ACJ injuries. Similarly no operation is without the potential for complications. Around 10% of people with grade 3 injuries treated with non operative treatment will have persistent problems with the upper limb and good reconstructive options remain if not healing well eg.(modified weaver Dunn). The only thing you lose with non operative treatment is time. Surgery is not the perfect solution for grade 3 ACJ injuries either, around 10% of operatively treated grade 3 injuries will have some form of problem. (See operative treatment) Grade 4 and 5 injuries are less likely to settle with non operative treatment and as such surgery might be a better option early on. Having said that, it is still possible to treat it non operatively in the first instance. The bump/ deformity will never disappear but it is surprising what good function can be achieved with non operative treatment. It is always possible to do a later reconstructive procedure if the arm function is not satisfactory. The problem with the higher grade injuries is less people will do well with non operative treatment and as such on balance in some cases, if time is of the essence and high level overhead shoulder function is needed, it may be better to operate early. Several variables need to be considered when treating these injuries (See operative treatment) Grade 6 injuries are extremely rare and require surgical treatment.Non operative treatment
Non operative treatment involves relative rest, analgesia and sensible use of the arm till the ligaments heal. Relative rest - muscle ligaments and bones like a little movement while healing and will ultimately heal stronger if gently stressed while healing. However if you keep overdoing it, it will slow the healing process down. Listen to your shoulder, not literally but figuratively - "If it hurts you are doing too much, if not you are doing too little. Don't do nothing , keep the range of motion in your shoulder gently stretch it a few times a day. Use a broad arm sling to support the arm when aching and to stop you from swatting a fly and grabbing a falling cup. Discard the sling as the shoulder settles and pain reduces. Ligaments take time to heal, around 4-8 weeks.Operative treatment
Several options have been tried to solve the problem of ACJ dislocation, some listed below: K - Wires Bosworth screw Hook plate Nottingham sling (Surgilig) Tightrope (open and all arthroscopic) Artificial ligaments (Lars ligament) Ligament reconstruction (Hamstring autograft) K wires Of all the surgical options this method is not advisable. Although it is possible to simply reduce the collar bone down to the acromion and then pass wires percutaneously through the skin. This method is not secure enough and the complication rate includes migration of the wires. Bosworth screw In an attempt to obtain more secure fixation, a screw is placed through the clavicle into the coracoid. The problem with this is, elevation of the arm above shoulder height induces a rotational force on the clavicle which would lead to loosening and fatigue failure of the screw. A drill hole into the base of the coracoid also weakens the coracoid and could lead to coracoid fracture. A coracoid fracture is very difficult to deal with Hook plate The hook plate is a very powerful way of holding the clavicle reduced to the correct level alongside the acromion. The problem with the hook plate is it requires removal at a later date as the hook under the acromion can cause problems with the tendons of the shoulder and with time can erode through the bone of the acromion. Hence it means 2 operations, one to insert and one to remove. The hook under the acromion may also limit arm movement above shoulder height till it is removed. The timing of removal is around 3 months following insertion. The clavicle may pop back up after removal if removed prior to sound ligament healing. Nottingham sling (Surgilig/ lockdown) In this procedure a synthetic ligament is looped around the coracoid and over the clavicle, holding the clavicle reduced to the level of the acromion. It is very effective and strong avoiding the problems of the hook plate. This strong construct may also create problems. In one of the original series of 11 patients, there was a coracoid fracture. (See references) Coracoid fractures are not easy to deal with. With such a strong permanent structure any further trauma to the shoulder must dissipate through the coracoid or the clavicle. Tightrope/ twin tails It is possible to reconstruct the coracoclavicular ligaments with synthetic suture material (fibrewire). It is possible to insert this in an all arthroscopic way or open. A hole is drilled in the clavicle and coracoid base and the fibrewire passed through the holes. The fibrewire is secured under the coracoid and above the clavicle with a button. Although it is possible to do this all arthroscopically and with small incisions, it is a technically demanding procedure. It requires drilling a hole in the base of the coracoid. This weakens the coracoid and if multiple passes are used with the guide wire or the coracoid is drilled eccentrically it can significantly weaken the coracoid. The single strand construct may also fatigue fail, hence the double strand construct was devised. This also replicates normal anatomy, the CC ligament composed of two distinct strands. Although this is mechanically much stronger the risk of coracoid fracture remains. A coracoid fracture although rare is difficult to deal with. The larger the hole in the base of the coracoid the greater the risk of fracture. Artificial ligament Very similar to the nottingham sling or surgilig there are different artificial synthetic ligaments to reconstruct the coracoclavicular ligament eg Lars ligament. These are very strong and loop around the under surface of the coracoid, the risk remains with the rigid construct of coracoid fracture. Ligament reconstruction (hamstring autograft) It is possible to reconstruct the coracoclavicular ligaments with natural tendons, either from a donor (allograft) or from your own body (autograft). Very similar to the way the anterior cruciate ligament in the knee is reconstructed. This biological reconstruction is less rigid than the artificial ligaments, but carries all the risks and problems of tendon grafts. Where the tendon is attached to the bone is also through bone tunnels, these are weak points in the coracoid and clavicle and could lead to fractures later on. In summary there are several surgical options available none perfect for everyone, each with there own pro's and con's. Treatment whether non operative or operative is very much an individual decision based on the severity of the injury and the patients expectations and needs.Outcome
The outcome is very variable, most grade 1 and 2 injuries settle with non operative treatment. Most Grade 3 injuries settle with non operative treatment, and those that don't it is still possible to undertake reconstruction at a later date with a modified weaver dunn procedure. In grade 4 and 5 injuries the outcome is more variable and often early surgery is advisable.References
Chronic acromioclavicular separation: the medium term results of coracoclavicular ligament reconstruction using braided polyester prosthetic ligament. Jeon IH, Dewnany G, Hartley R, Neumann L, Wallace WA. Injury. 2007 Nov;38(11):1247-53 In this series, we treated chronic acromioclavicular disruption with an artificial coraco-clavicular ligament made from braided polyester (The Nottingham Surgilig). The ligament has a loop at each end and is passed around the coracoid process, threaded through itself, then passed around the posterior aspect of the clavicle and finally anchored to it with a bone screw. Eleven men with an average age of 39 underwent this procedure. Three patients had previously been operated on using the Weaver—Dunn procedure which had failed. All eleven patients have been reassessed clinically and radiographically at an average of 55 months. Using the Imatani evaluation score, 10 patients achieved a good/ excellent result with the mean Constant score being 92. One patient had fracture of the base of the coracoid after heavy lifting in the early postoperative period which resulted in a poor outcome. Two patients needed an additional operation. In one the lateral end of the clavicle was excised together with removal of the fixation screw, and in the other a subacromial decompression was carried out. The Nottingham Surgilig is a useful alternative for the treatment of chronic acromioclavicular separation, especially in revision reconstruction when the coracoacromial ligament is no longer available.