Ankle block
Anatomy:
The terminal branches of sciatic and femoral nerve supply the ankle
joint.
The sciatic nerve divides into tibial nerve and common peroneal or fibular
nerve.
Branches of the tibial and common peroneal nerve form the sural nerve.
The only branch of the femoral nerve which contributes to sensory
innervation below the knee is the saphenous nerve.
The saphenous nerve supplies
the skin on the medial aspect of the ankle joint.
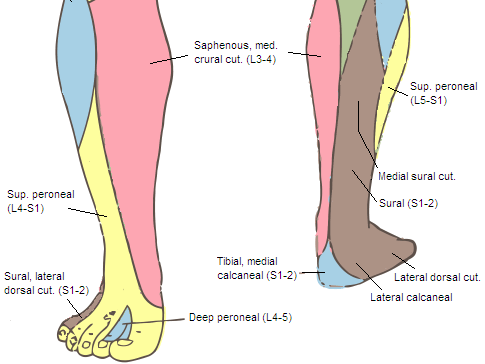
Sensory innervation of ankle:
The images below are a rough guide.
There is normally a considerable overlap between the nerves.
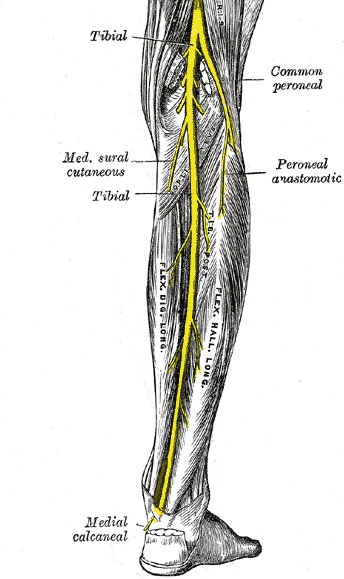
Tibial nerve:
The tibial nerve descends though the middle of the popliteal fossa,
posterior to the popliteal vein and artery (when scanning from behind it
is more superficial compared to the blood vessels).
In the leg it is
accompanied by posterior tibial artery.
The tibial nerve leaves the
posterior compartment of the leg by passing deep to the flexor
retinaculum between the medial malleolus and calcaneum.
The tibial
nerve lies between the posterior tibial vessels and the tendon of the
flexor hallucis longus.
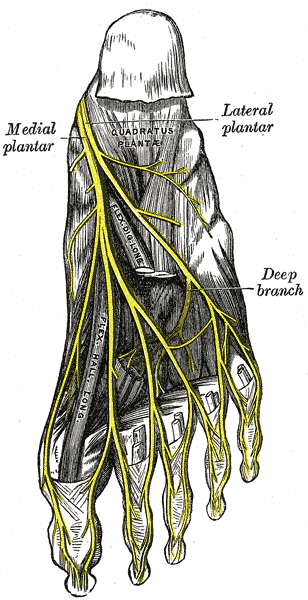
Tibial nerve divides into the medial and
lateral plantar nerves.
Common peroneal nerve:
The common peroneal nerve is one of the terminal
branches of the sciatic nerve. It begins in the popliteal fossa
and runs along the medial border of the biceps femoris muscle. It exits
the popliteal fossa by passing over the lateral head of the
gastrocnemius muscle.
The common fibular nerve then goes around the
neck of the fibula uder the peroneus longus muscle and then divides into
the superficial and deep peroneal nerves.
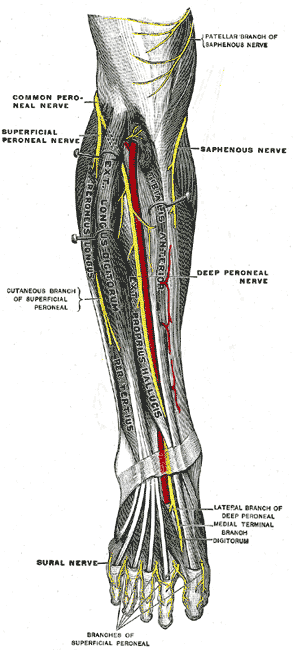
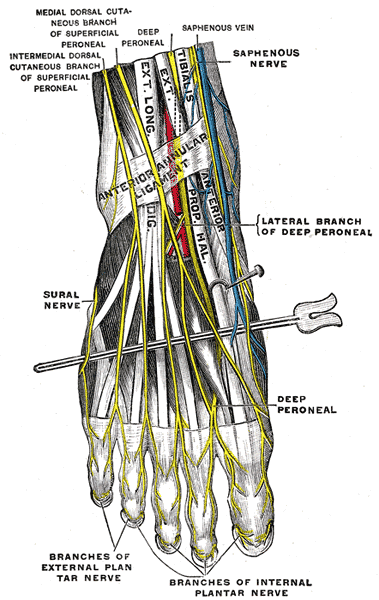
Deep peroneal nerve:
The deep peroneal nerve begins deep to the peroneous (fibularis) longus muscle and then passes under the
extensor digitorum longus.
It pierces this to lie anterior to the interosseous
membrane.
It then accompanies the anterior tibial artery between the extensor
hallucis longus and tibialis anterior muscles.
Superficial peroneal
nerve:
This nerve begins between the peroneus longus muscle and the fibula. It
then passes anterolateral to the fibula between the peroneous longus muscles and
the extensor digitorum longus which it supplies along with peroneous brevis.
It
pierces the deep fascia at the lower third of the leg.
It passes in the
superficial fascia to supply the skin on the distal part of the anterior surface
of the leg, nearly all the dorsum of the foot and most of the digits.
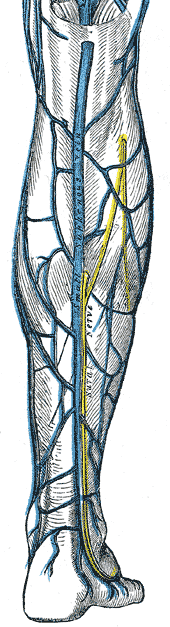
Sural nerve:
This is formed from a contribution by the tibial (the medial sural cutaneous nerve) and the
common peroneal nerve (sural communicating branch).
This nerve supplies the skin
of the posterolateral side of the inferior third of the leg and the lateral side
of the foot.
The Sural nerve lies behind the lateral malleolus along with the short
saphenous vein.
It supplies the posterior part of the sole, the back of the lower leg, the heel and lateral side of the
foot.
Saphenous nerve:
The Saphenous nerve is the
only sensory contribution of the femoral nerve below the knee joint. It arises from
femoral nerve in the femoral triangle and descends through it on the lateral side of the
femoral vessels to enter the adductor canal behind its aponeurotic covering.
At
the lower part of adductor magnus it separates from the artery behind the
sartorius muscle. On the medial side of the knee it emerges by piercing the
fascia lata between sartorius and gracilis to lie in the subcutaneous plane.
In
the leg the saphenous nerve follows great saphenous vein.
Indications of ankle block:
Any surgery below the level of
ankle joint: midfoot and forefoot surgery.
It can be combined with an ankle
tourniquet.
Advantage is that it avoids foot drop and thus patient can be
mobilized immediately after surgery.
Bilateral ankle blocks can be carried out without affecting mobilization.
It provides analgesia for up to 18-24 hours after surgery.
Contraindications of ankle block:
1. Patient refusal.
2. Infection at the site of injections.
This involves multiple injections
and a good amount of sedation will improve patient comfort.
Key points:
1.
It is not necessary to block all five nerves. Choose the nerves to be blocked
depending on the site of surgery.
2. Like with any other ultrasound
technique follow the structure which you think is a nerve proximally and
distally along the leg to confirm that it is actually a nerve.
See how it
behaves in relation to other structures.
3. Four out of five nerves lie
close to blood vessels.
4. Nerves are scanned cephalad to the ankle joint. It
is very difficult to scan around the ankle joint as the ultrasound probe cannot make
good contact with the skin around the ankle.
Necessary
Equipment:
1. Ultrasound machine with high frequency probe, probe cover and
ultrasound gel
2. Insulated stimulating needle (I use 50 mm stimulating
needle: only the posterior tibial nerve can be stimulated, it produces toe plantar
flexion on stimulation. The other nerves do not produce any motor response at this
level).
3. 23G Hypodermic needle to block other four nerves.
4. Local
anaesthetic: 5 ml per nerve of 0.5% levobupivacaine
5. 2%
chlorhexidine
Locating and blocking the nerves:
In the following two videos Dr Anthony Allen explains how to
locate five nerves carrying sensation form the ankle and his
technique of blocking them.
Ankle block part 2
Following video is courtesy 'Nerve imaging group' and can be
seen on RA-UK website.


