Femoral Block
Anatomy
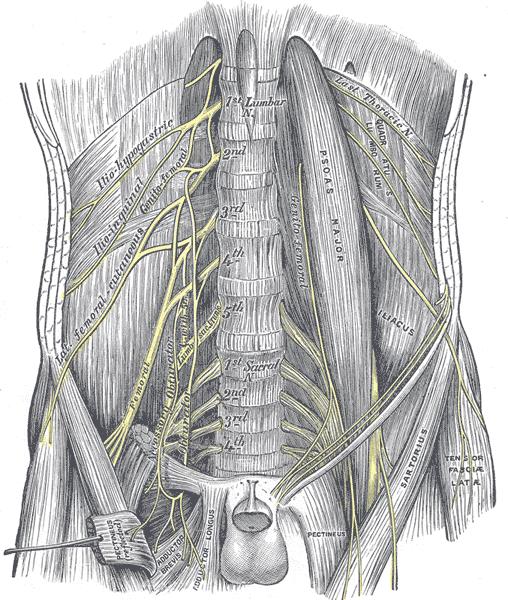
The femoral nerve is a branch of lumbar plexus. It arises from L2 to L4
lumbar nerves. It descends through the fibers of the psoas major muscle and
then is positioned between it and the iliacus muscle. Here it is covered by
the iliac fascia. It then passes under the inguinal ligament. It then
divides into anterior and posterior division. It lies on the lateral side of
the femoral artery separated from it by iliac fascia. The anterior division
gives rise to muscular branch (Sartorius and pectineus muscle) and cutaneous
branches (medial and intermediate cutaneous nerves of thigh). Posterior
division gives rise to muscular branches to quadriceps muscles and articular
branches to the hip and knee joint. Articular branches are given by nerves to
the quadriceps muscle.
Anatomy relevant to the block:
The red line shows the
level of the inguinal ligament. However the level of inguinal crease is
much lower than that. You will note that in the picture at the level of inguinal ligament a
single femoral nerve lies lateral to the single femoral artery.
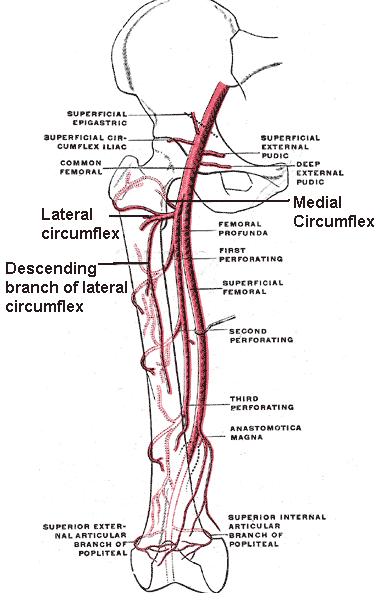
However
both femoral nerve and artery start to divide into multiple branches as soon
as they pass under the inguinal ligament. Femoral artery will divide into
superficial and deep femoral artery. Lateral femoral circumflex artery (LFCA)
arises from the deep femoral artery. LFCA may lie between the branches of
femoral nerve. At the level of inguinal crease more than one femoral artery
may be seen.
Femoral nerve also divides extensively below the inguinal
ligament. We have discussed the branches before. In an interesting paper
published in 2010, Kenneth J et al looked at the fascicular anatomy of the
femoral nerve. They dissected eight femoral nerves in four female cadavers.
They found the distance from the inguinal ligament to the first branching
point of the femoral nerve was 1.50 ± 0.47 cm (range 1–2cm). Most branching
occurred within a small length of the nerve. Branches to the pectineus muscle,
sartorius muscle, and sensory nerves (saphenous and medial cutaneous) branched
first and medially in seven out of eight specimens. In all but one specimen,
the branch to the sartorius originated on the ventral surface. The branches
innervating vastus medialis, vastus intermedius, and vastus lateralis muscles
were centrally located and the branch to rectus femoris muscle was lateral in
the branching pattern of all specimens. The femoral nerve was an elongated
ellipse rather than circles. Femoral nerve width was almost five times the
height thus was a more flattened structure. This paper is available on
the internet:
http://www.rehab.research.va.gov/jour/09/46/7/pdf/gustafson.pdf
So when ultrasound probe is
placed below the inguinal crease you may see more than one artery or nerve.
Moving the probe cephalad as shown will result in visualization of single
artery and nerve.
Femoral nerve lies underneath the iliac fascia.
The following video shows the ultrasound anatomy of the femoral nerve.
It is the main nerve above the knee. Below the knee the main nerve is sciatic
nerve. Obturator nerve plays a small part on the medial side of the knee. br
Indications:
1.Providing postoperative analgesia for surgery on knee and hip joint (e.g. knee
replacement, hip replacement).
2.Femoral fracture surgery: Very good
for providing pain relief. Beneficial opioid sparing effect in elderly.
3.Above knee amputation for pain relief. Femoral nerve is the major
component above the knee. It plays a smaller role in providing pain relief
following below knee amputation. Sciatic nerve plays a greater part below the
knee.
Contraindications: Absolute contraindications are patient refusal and
infection at the site of femoral nerve block.
Equipment
1.Ultrasound
machine with high frequency linear probe
2.Stimuplex or equivalent 100
mm needle
3.Chlorhexidine 2% for asepsis
4.Local anaesthetic:
For providing analgesia I use 0.25% levobupivacaine 20 ml. If I do the block
for providing anaesthesia then I use a higher concentration of local
anaesthetic.
Technique:

Patient lies supine. Anaesthetist stands on the side of the patient the
block is going to be done. The machine is positioned as shown in the picture
so that everything is easily visible and accessible to the anaesthetist
picture Ultrasound probe is placed below the inguinal crease and parallel to
it so that a cross sectional view of a single femoral artery is obtained.
If more than one artery is seen the probe is moved cephalad till a single
artery is seen. At this point femoral nerve is located lateral to it.
Femoral nerve may be seen as a single structure or may have already divided
into two divisions or multiple branches. In that case an attempt is made
to see a single nerve or to see the two divisions very close. Sometimes
if the patient is obese then it is not possible to move the probe cephalad
in that case best possible view of the nerve or its divisions is obtained.
Needle is introduced in-plane so that the needle is seen approaching the nerve
from lateral side. The aim is to surround the nerve (or the divisions)
with local anaesthetic. If nerve stimulator is used I have
observed that when the needle is close to the posterior division a
patellar twitch is seen and when the needle is closer to anterior division
then a twitch of the Sartorius muscle is seen.
Following video is from RA-UK. It shows in-plane ultrasound guided
femoral nerve block
Video. 

