Elbow block
Following nerves can be blocked at the level of elbow:
Median nerve
Radial nerve
Ulnar nerve
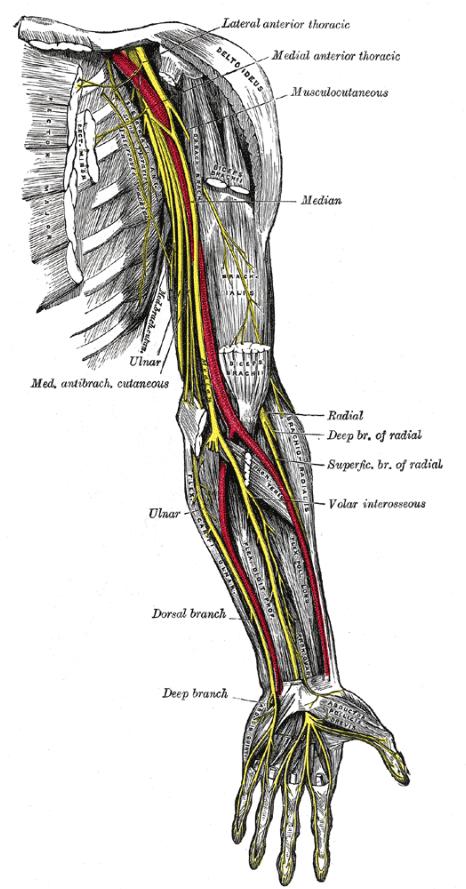
Median Nerve:
Anatomy
The
Median nerve lies on the medial side of the brachial artery at the level
of elbow crease.
This image is from Gray's anatomy
and shows median nerve lying medial to the artery at the level of elbow.
Locating the nerve:
Use a linear high frequency transducer.
Position it just above the
elbow crease so as to obtain a cross sectional view of the brachial
artery.
Do not look for the nerve initially. Find the
artery, then look medial to the artery.
The Nerve lies medial to the
artery.
You will have to adjust the probe (tilting and clockwise and
counterclockwise movement) to get the best view of the nerve.
Most of
the time it is quite closely associated with the artery but sometimes it
can be further away.
The best way to confirm it is the nerve is to scan back
towards the axilla. The median nerve always stays with the artery and
if it is further away at the elbow then it will join the artery by midarm
level.
Mobile users please click here for
video
Anisotropy demonstrated by median nerve at midforearm level
Indication:
1.To supplement an incomplete
brachial plexus block done proximally
2.To provide postoperative
analgesia
Contraindications:
1.Patient refusal
2.Infection
at the site of block
3.Coagulopathy
Equipment:
1. Ultrasound machine with high frequency linear transducer.
2. Probe cover with ultrasound jelly
3. 50 mm insulated stimulating needle with a nerve stimulator
4. 5 ml of 0.5% or 0.25% levobupivacaine.
Performing the nerve block:
After intravenous access is established and
appropriate monitoring used.
Patient, anaesthetist and the ultrasound
machine are positioned as shown in the picture.

The needle is inserted in-plane so that the entire needle is visualised
as it approaches the nerve.
You may do this block without
a nerve stimulator but it is our practise to combine both techniques.
The nerve stimulator is set to deliver a current of 0.5mA.
The
needle at first is directed above the nerve and local anaesthetic is
injected above it.
Then the needle is directed below the nerve and
local anaesthetic injected below the nerve.
In case the needle
produces motor stimulation (finger flexion/wrist flexion/supination)
then the current is reduced so that no motor stimulation is produced at
current less than 0.2mA.
Also the twitch should disappear as soon as
local anaesthetic is injected.
The local anaesthetic (shown
in blue) is
injected around the nerve as shown:
The following is video of a median nerve block. Video courtesy Nerve Imaging group and can also be found on RA-UK website
:
Ulnar
nerve block:
Anatomy:
The ulnar nerve emerges from behind the medial
epicondyle and descends on the medial side of the forearm.
At a
variable point in the forearm it is joined by ulnar artery. The ulnar
artery is formed by the division of brachial artery in front of elbow
into radial and ulnar artery.
The ulnar nerve lies on the medial side of
the ulnar artery.
The point at which they lie close to each other is highly variable.
This point can be high in the forearm or as low as just
above the wrist.
The following video demonstrates this
point. Both forearms of the same individual are scanned.
On scanning the
right hand you can see the nerve joining the artery at the level of
midforearm.
On the left hand side the artery does not join the nerve
till the level of wrist.
Scanning the right side first and then the left side
Locating the nerve:
Use a high frequency
linear transducer.
Place the probe over the midforearm level on medial
side so that a cross sectional view of the ulnar artery is visible.
Look at medial side of the artery. The nerve may be visible close to the
artery at this level.
If not scan towards the wrist maintaining the
cross section view of the artery in the middle of picture.
You will see
the nerve joining the artery from the medial side.
Once the nerve is
identified then trace the nerve all the way back to the elbow. See that
the nerve seperates from the artery and then descends towards the medial
epicondyle.
Indication:
1.To supplement an incomplete brachial
plexus block done proximally
2.To provide postoperative analgesia
Contraindications:
1. Patient refusal
2. Infection at the
site of block
3. Coagulopathy
Equipment:
1.Ultrasound
machine with high frequency linear transducer.
2.Probe cover with
ultrasound jelly
3.50 mm insulated stimulating needle with a nerve
stimulator
4.5 ml of 0.5% or 0.25% levobupivacaine.
Performing
the nerve block:
After intravenous access is established and appropriate
monitoring used.
Patient, anaesthetist and the ultrasound machine are
positioned as shown in the picture.

The needle is inserted in-plane
so that the entire needle is visualised as it approaches the nerve.
You may do this block without a nerve stimulator but it is our practise to
combine both techniques.
The nerve stimulator is set to deliver a
current of 0.5mA. The needle at first is directed above the nerve and
local anaesthetic is injected above it.
Then the needle is directed
below the nerve and local anaesthetic injected below the nerve.
In case
the needle produces motor stimulation (finger flexion on ulnar
side/ulnar deviation of wrist) then the current is reduced so that no
motor stimulation is produced at current less than 0.2mA.
Also the twitch should disappear as soon as local anaesthetic is
injected.
Following is the video of ulnar nerve block. Video courtesy Nerve
Imaging group and can also be found on RA-UK website :
Radial block:
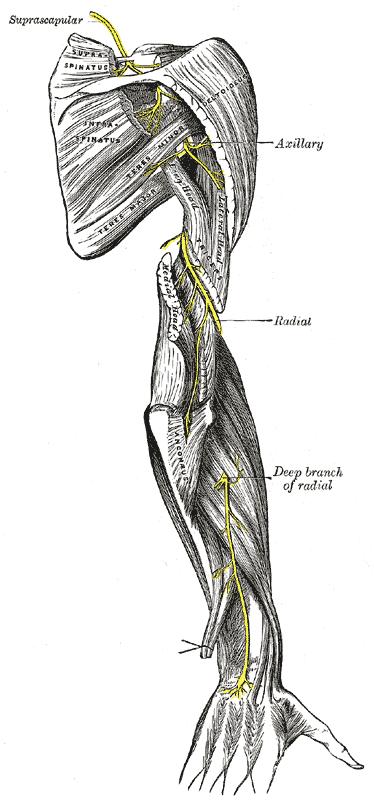
Anatomy
The radial nerve arises from the
posterior cord of the brachial plexus.
In the axilla the radial nerve is
with the axillary artery but goes posteriorly along the medial border of
the arm.
The radial nerve winds around the arm in the spiral groove
between medial and lateral heads of triceps.
The radial nerve then
emerges on the lateral aspect of the arm. Iit pierces the lateral
intermuscular septum at this point and then lies in the anterior
compartment of the arm.
It then travels between the brachialis and
brachioradialis muscles to the front of elbow.
Here it divides into
superficial and deep branch
Locating the nerve:
Use a high frequency linear transducer.
Start
scanning four finger breadths above the lateral epicondyle.
You will see
bony the shadow produced by the humerus.
The radial nerve will be seen just in
front of humerus.
As you follow the nerve towards the elbow you will
see it flattening out and then divide in front of the elbow into the
superficial and deep branch.
Indication:
1.To supplement an incomplete brachial plexus block done proximally
2.To provide postoperative analgesia
Contraindications:
1.Patient refusal
2.Infection at the site
of block
3.Coagulopathy
Equipment:
1. Ultrasound machine
with high frequency linear transducer.
2. Probe cover with
ultrasound jelly
3. 50 mm insulated stimulating needle with a nerve
stimulator
4. 5 ml of 0.5% or 0.25% levobupivacaine.
Performing
the block:
After intravenous access is established and appropriate
monitoring used.
Patient, anaesthetist and the ultrasound machine are
positioned as shown in the picture.

The needle is inserted in-plane so
that the entire needle is visualised as it approaches the nerve.
You
may do this block without a nerve stimulator but it is our practise to
combine both techniques.
The nerve stimulator is set to deliver a
current of 0.5mA.
The nerve is surrounded by local anaesthetic.
In
case the needle produces motor stimulation (finger extension) then the
current is reduced so that no motor stimulation is produced at current
less than 0.2mA.
Also the twitch should disappear as soon as local
anaesthetic is injected.
The following video is from RA-UK website of
ultrasound guided radial nerve block. It is courtesy of 'Nerve Imaging
Group'.


